Ringing in the ears after a loud concert is common. Ringing that has been present, every day, for three years is an entirely different clinical situation. Clinicians draw a line between these two states, not arbitrarily, but because the underlying biology and the realistic management options change as tinnitus persists.
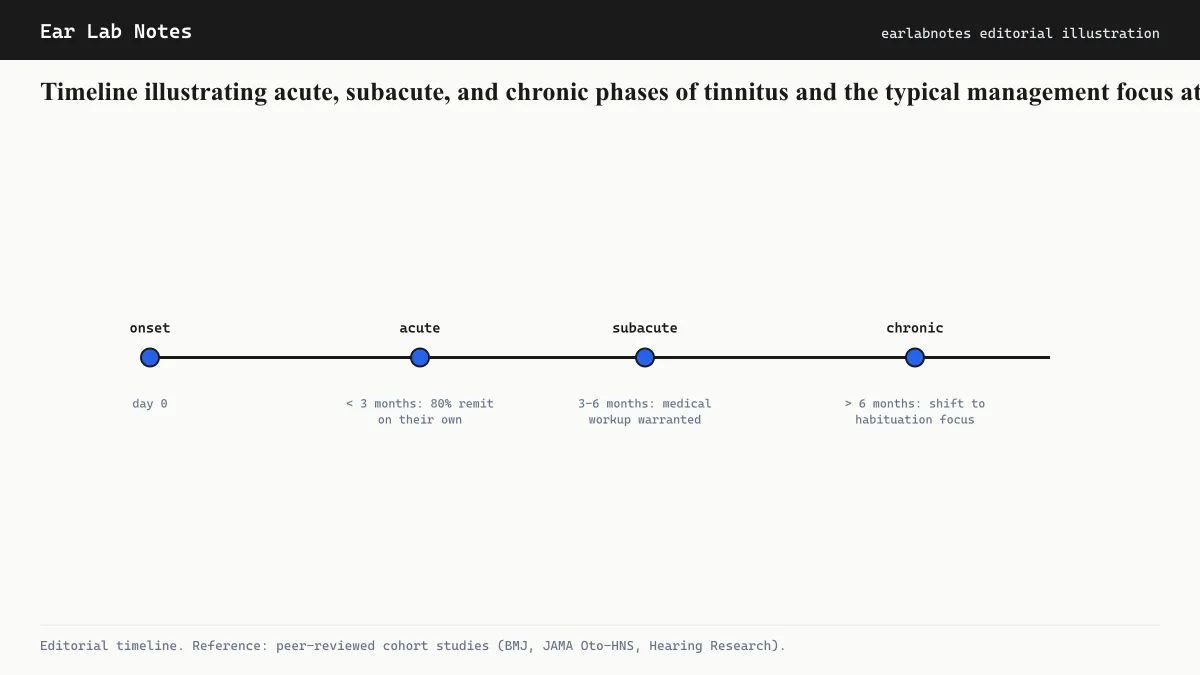
The most widely used classification divides tinnitus into three phases: acute, subacute, and chronic. Understanding which category applies matters when evaluating treatment options, prognosis, and the urgency of specialist referral.
The three phases
Acute tinnitus: zero to three months
Acute tinnitus is generally defined as tinnitus present for fewer than three months. This phase includes the most common scenario most people encounter: the ringing after a loud event that fades within hours or days.
During this window, the auditory system is often still recovering from whatever triggered the tinnitus, whether that is noise exposure, a medication side effect, a middle-ear infection, or barometric pressure changes during a flight. The brain’s auditory network has not yet had time to entrench the signal into long-term patterns of neural firing.
The NIDCD notes that temporary tinnitus after noise exposure is extremely common. Most of it resolves without intervention. When it does not resolve within two weeks, evaluation becomes appropriate.
Subacute tinnitus: three to six months
Some guidelines include a subacute category for tinnitus between three and six months in duration. During this window, the tinnitus has lasted long enough that spontaneous resolution is becoming less likely, but management strategies aimed at influencing the condition’s trajectory may still have meaningful potential.
Not all clinical frameworks use this middle category. The AAO-HNS and some European guidelines fold this period into chronic, while others treat it as a distinct phase with its own management emphasis.
Chronic tinnitus: beyond six months (some guidelines: three months)
Chronic tinnitus is the term for persistent tinnitus that has stabilized into a long-term pattern. The AAO-HNS guideline uses six months as the threshold, while some other frameworks use three months. The core idea is consistent: at some point, the neural processes underlying tinnitus have become sufficiently established that the management goal shifts.
Rather than trying to eliminate the tinnitus signal, chronic tinnitus management focuses on reducing the distress associated with it, improving sleep, concentration, and emotional wellbeing, and building the auditory habituation that allows many people to notice the tinnitus less over time.
Why the classification changes what clinicians do
Acute: find and address reversible causes
The primary task in acute tinnitus is identifying whether there is a reversible underlying cause. This is the phase where conditions like impacted cerumen, otitis media, sudden sensorineural hearing loss, or a recently started ototoxic medication may be contributing. Addressing these can resolve or significantly reduce the tinnitus.
Sudden sensorineural hearing loss, which often presents with tinnitus, is treated as an urgent matter. The NHS UK identifies it as a condition requiring prompt evaluation, as some treatments are most effective within a narrow time window.
Subacute: counseling and early habituation support
During the subacute phase, when spontaneous resolution remains possible but is no longer the default expectation, clinicians often introduce educational counseling about tinnitus mechanisms, reassurance where appropriate, and initial sound enrichment strategies. Some research groups are investigating whether early CBT-based interventions during this phase can reduce the proportion of patients who develop long-term distress, though this remains an active area of study rather than settled practice.
Chronic: distress reduction and function
Once tinnitus is clearly chronic, the evidence base for treatment converges on two main approaches: cognitive behavioral therapy (CBT) and sound-based interventions. The AAO-HNS guideline recommends offering sound therapy or structured CBT, or both, for patients with bothersome chronic tinnitus.
“Bothersome” is a key word here. Chronic tinnitus is extremely common. The NIDCD estimates that about 15 percent of the general public experience some tinnitus, and most of those people are not substantially disabled by it. Clinical management is focused on those for whom the tinnitus is interfering with daily function, sleep, or emotional health.
Prognosis: what duration predicts
Duration is one of the stronger predictors of whether tinnitus is likely to change significantly. Tinnitus that has been present and stable for a decade is unlikely to resolve spontaneously. Tinnitus that appeared three weeks ago has a much more variable trajectory.
This does not mean chronic tinnitus is untreatable. It means the goal of treatment is different. Habituation, the process by which the auditory system and brain gradually reduce the attention allocated to the tinnitus signal, can occur at any stage. The BTA notes that many people with long-standing tinnitus report significant improvement in their relationship to the sound over time, even when the sound itself does not change.
Factors that can influence progression
Several factors are associated with worse outcomes or persistence:
- Coexisting hearing loss (especially if untreated)
- High anxiety or catastrophizing responses to the tinnitus
- Sleep disruption that creates a feedback loop
- Absence of any explanation or counseling about the condition
- Continued noise exposure that may compound the underlying cause
Each of these can be addressed with appropriate support, which is part of why early audiological evaluation is recommended even for tinnitus that seems mild.
When to seek evaluation regardless of duration
The AAO-HNS identifies presentations that warrant prompt referral regardless of how long the tinnitus has been present. These include tinnitus that is unilateral, pulsatile, rapidly changing, or accompanied by neurological symptoms, vertigo, or sudden hearing loss.
For tinnitus that does not involve these features, the guidance is generally to seek evaluation if the tinnitus has persisted beyond two to four weeks or if it is interfering with sleep or daily activities.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- How long does tinnitus typically last after loud noise exposure?
- Temporary tinnitus after a single loud-noise event (a concert, a gunshot) often resolves within hours to a few days. If it persists beyond two weeks, evaluation by an audiologist is advisable. Persistence at that point may indicate underlying cochlear damage rather than a transient response.
- Does chronic tinnitus ever go away on its own?
- Spontaneous resolution of chronic tinnitus (present for more than three months) does occur but becomes progressively less common the longer the tinnitus persists. Many people find that while the sound itself may not disappear, habituation reduces how much it intrudes on daily life. An audiologist can explain what outcomes are realistic for a given presentation.
- What is the three-month threshold based on?
- The three-month cutoff is a clinical convention rather than a hard biological boundary. It reflects the observation that most tinnitus with a chance of spontaneous resolution will have resolved within that window, and that neural habituation and cortical reorganization become progressively more entrenched after that point. Some guidelines use six months as the threshold for chronic classification.
- Does treatment work differently for new versus long-standing tinnitus?
- Emerging evidence suggests that interventions during the acute period may have better potential to influence the trajectory. Some researchers are investigating whether early sound therapy or counseling can reduce the transition to chronic distress, though this area is still under study. For chronic tinnitus, management focuses primarily on reducing distress and improving function rather than eliminating the sound.
Primary sources
Where this comes from
- ◆ Clinical Practice Guideline: Tinnitus · American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- ◆ Tinnitus · NIH/NIDCD
- ◆ Tinnitus: causes and management · NHS UK
- ◆ About Tinnitus · British Tinnitus Association (BTA)
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N001 · The Ear Lab · earlabs.app