Among the many interventions studied for chronic tinnitus, cognitive behavioral therapy (CBT) has the most consistent and substantial evidence base. The AAO-HNS (American Academy of Otolaryngology) clinical practice guideline on tinnitus recommends CBT as an effective management option for patients with bothersome chronic tinnitus. The NHS UK lists it among the primary recommended approaches.
This matters because tinnitus is a condition that receives an enormous volume of marketing for supplements, devices, and programs with little or no supporting trial data. CBT is the exception: a structured psychological approach with a meaningful body of randomized controlled trial evidence behind it.
Understanding what CBT for tinnitus actually involves, what outcomes trials demonstrate, and what it does not do helps people make informed decisions about management.
What CBT does and does not do
The most important thing to understand about CBT for tinnitus is that it does not target the acoustic signal.
Tinnitus loudness, measured objectively through audiological pitch and loudness matching, does not consistently change after CBT. Multiple trials confirm this: the sound itself typically stays the same.
What changes is the distress. Trials of CBT for tinnitus consistently show reductions in tinnitus-related anxiety, depression, intrusion, and quality-of-life impairment. Many participants also report perceiving the tinnitus as less loud or less intrusive, even when objective loudness measurements do not change.
This discrepancy reflects how significantly attention, emotion, and interpretation shape the perception of tinnitus. The acoustic signal is the same; the meaning and attention given to it drive much of the suffering.
The CBT model of tinnitus distress
CBT for tinnitus is built on a specific model of how distress develops and maintains itself.
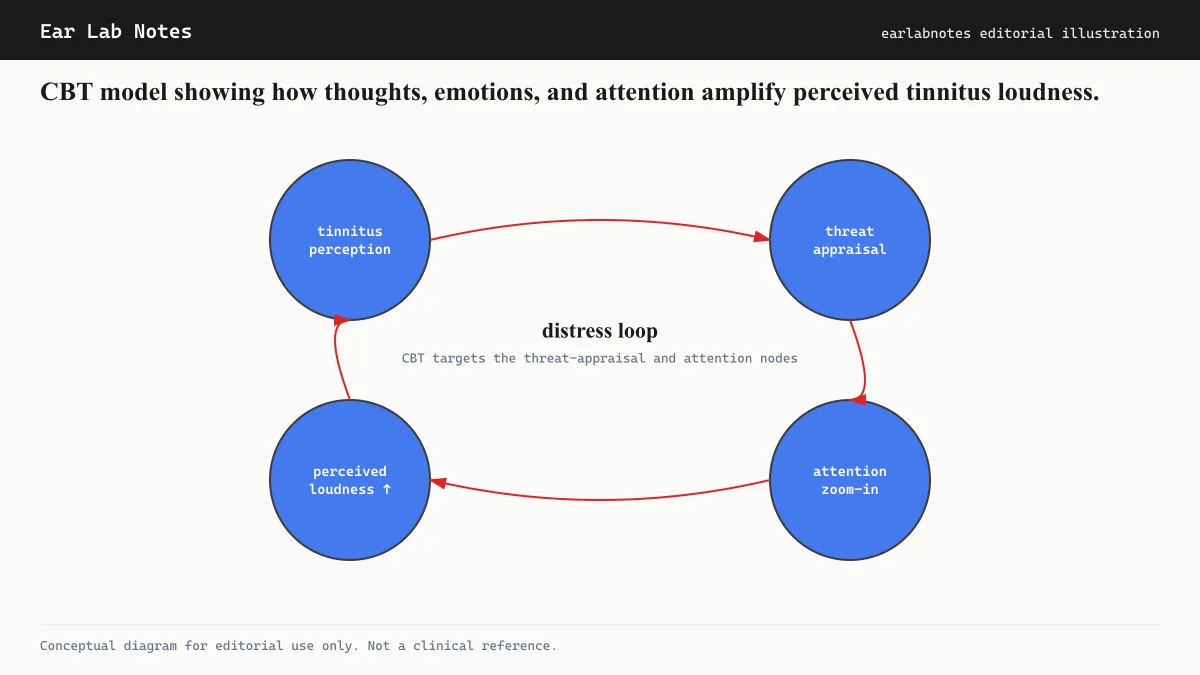
The model proposes a feedback loop:
- The tinnitus signal is detected by the auditory system
- The brain’s threat-monitoring system, centered on the amygdala and limbic system, evaluates the signal
- When the signal is appraised as threatening, dangerous, or a sign of serious illness, this appraisal triggers anxiety and increased attention to the tinnitus
- Increased attention and negative emotion amplify the perceived loudness and salience of the tinnitus
- This amplified experience reinforces the belief that the tinnitus is serious, completing the loop
CBT intervenes at multiple points in this cycle: changing the appraisal (the meaning given to the tinnitus), reducing attentional bias toward the sound, and modifying the behavioral responses (such as avoidance of situations or sounds) that maintain distress.
What happens in CBT for tinnitus
A standard CBT-for-tinnitus protocol typically runs between 6 and 12 sessions. The structure varies by program but generally includes the following components.
Psychoeducation
The first sessions typically focus on explaining what tinnitus is, how it is generated, and why the distress model described above means that changing thoughts and behaviors can genuinely change the experience. Many patients arrive with fears that tinnitus indicates a brain tumor, impending deafness, or a condition that will inevitably worsen. Evidence-based psychoeducation addresses these directly.
The NHS and BTA both provide patient-facing educational materials about tinnitus that align with this element of CBT, though formal CBT replaces passive information with active behavioral practice.
Identifying and monitoring automatic thoughts
Patients learn to notice the automatic negative thoughts that arise in response to tinnitus. Common examples include “I will never be able to sleep properly again,” “this is going to ruin my life,” or “something must be seriously wrong.” These thoughts occur quickly and automatically, and most people have not previously examined them critically.
Recording these thoughts (often in a thought diary) makes them visible and workable.
Cognitive restructuring
Cognitive restructuring is the process of examining automatic thoughts and testing their accuracy. This involves identifying cognitive distortions (catastrophizing, all-or-nothing thinking, mind reading), evaluating the evidence for and against the thought, and developing more realistic alternatives.
This is not positive thinking. It is a systematic examination of whether the thought is actually supported by evidence. “I will never sleep again” can be tested against the patient’s own history of sleep since the tinnitus began.
Behavioral experiments and exposure
Avoidance is a central maintaining factor in tinnitus distress. Patients who avoid quiet environments (because silence makes tinnitus more prominent), social situations, or activities they previously enjoyed deprive themselves of evidence that those situations are manageable. They also reinforce the belief that the tinnitus is dangerous.
Behavioral experiments involve deliberately approaching avoided situations to test predictions. The data collected from these experiments become evidence in the cognitive restructuring process.
Attention training
Tinnitus draws attention involuntarily, especially when the brain has tagged it as important. Attention training exercises aim to develop greater voluntary control over where attention is directed, reducing the automatic capture of attention by the tinnitus signal.
Relapse prevention
The final sessions typically focus on consolidating skills and preparing for periods when tinnitus distress may spike (during illness, stress, or poor sleep). This includes developing a personal plan for managing difficult periods.
Who delivers CBT for tinnitus
CBT for tinnitus is most effective when delivered by therapists with specific training in tinnitus management. This may include clinical psychologists, psychotherapists, audiologists with psychological training, or hearing therapists who have completed specialist tinnitus programs.
The AAO-HNS recommends referral to appropriate specialists for patients who would benefit from CBT. Finding a qualified provider may require some searching, as tinnitus-specific CBT is not yet universally available.
Internet-delivered CBT programs for tinnitus have been studied in multiple randomized trials. Results generally show meaningful reductions in tinnitus distress comparable to face-to-face delivery, with the advantage of accessibility. Several programs have been developed and tested in Scandinavian and UK research centers.
What CBT does not replace
CBT addresses the psychological and attentional aspects of tinnitus distress. It does not replace audiological evaluation, which is needed to identify any treatable underlying causes and to assess hearing loss. Sound therapy, hearing aids, and other audiological interventions address different aspects of the problem and are often combined with CBT.
The Mayo Clinic and NIDCD both note that tinnitus management is most effective when multiple dimensions (audiological, psychological, and behavioral) are addressed in a coordinated way.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- Does CBT make the tinnitus quieter?
- CBT for tinnitus does not typically reduce the acoustic loudness of the tinnitus when measured objectively. What multiple trials show is a significant reduction in tinnitus-related distress, depression, anxiety, and the impact on daily functioning. Many people report perceiving the tinnitus as less intrusive after CBT, even when the signal itself has not changed measurably. This distinction is clinically important.
- How many sessions of CBT does tinnitus treatment require?
- Most structured CBT-for-tinnitus programs run between 6 and 12 sessions, with 8 sessions being a common protocol length. Some internet-based programs deliver similar content in a self-paced format over 8 to 12 weeks. Session frequency and format depend on the specific program and provider. Consult an audiologist or psychologist trained in tinnitus CBT for guidance on what is appropriate for your situation.
- Is CBT for tinnitus the same as CBT for anxiety or depression?
- CBT for tinnitus borrows heavily from standard CBT techniques but is adapted specifically to the cognitive and behavioral patterns associated with tinnitus. This includes psychoeducation about tinnitus mechanisms, attention retraining, addressing catastrophizing thoughts about the tinnitus, and behavioral experiments related to sound avoidance and activity withdrawal. A therapist with specific tinnitus training is generally more effective than general CBT.
- Is internet-based CBT for tinnitus effective?
- Several randomized controlled trials have evaluated internet-delivered CBT programs for tinnitus. Results generally show effect sizes comparable to face-to-face CBT, with the added advantage of accessibility for people who cannot easily attend in-person sessions. The NHS in the UK has published guidance on digital mental health approaches for tinnitus. Consult with an audiologist about which format may be suitable.
- Does CBT work for everyone with tinnitus?
- No single treatment works for all people with tinnitus. CBT is more likely to produce meaningful benefits in those experiencing significant tinnitus-related distress, anxiety, or depression. People with mild tinnitus that is not significantly affecting their life may not need or benefit from formal CBT. An audiologist or clinical psychologist can help determine whether CBT is a good fit.
Primary sources
Where this comes from
- ◆ Tinnitus · NIH/NIDCD
- ◆ Clinical Practice Guideline: Tinnitus · American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- ◆ Tinnitus: causes and management · NHS UK
- ◆ Tinnitus · Mayo Clinic
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N007 · The Ear Lab · earlabs.app