When people describe tinnitus as ringing, they are most often describing high-frequency tinnitus. A sharp, persistent tone sitting somewhere between 4,000 Hz (4 kHz) and 8,000 Hz (8 kHz) is the most common pitch reported in clinical tinnitus populations. This range is not a coincidence. It reflects the frequency region where cochlear damage tends to begin, whether from noise exposure, aging, or a combination of both.
Understanding why this frequency range is affected first helps explain why high-pitched tinnitus is so prevalent, and why the noise notch on an audiogram tells a specific story about how the damage occurred.
The anatomy of vulnerability at 4 kHz
The cochlea encodes sound frequency along its length, a property called tonotopy. High frequencies are processed at the base, low frequencies at the apex. The 4 kHz region falls in the basal portion of the cochlea, which is the zone of highest mechanical stress when the ear is exposed to sounds in the midrange of human hearing.
NIOSH (the National Institute for Occupational Safety and Health) and the NIDCD both identify 4 kHz as the frequency where noise-induced hearing loss characteristically first appears. Several factors converge to make this region particularly vulnerable:
- The traveling wave set up by incoming sound reaches peak amplitude in this region for many common noise frequencies
- The blood supply to the basal cochlea is somewhat less robust than to the apex
- Outer hair cells in this region appear to be more susceptible to metabolic overload from acoustic overstimulation than those in adjacent regions
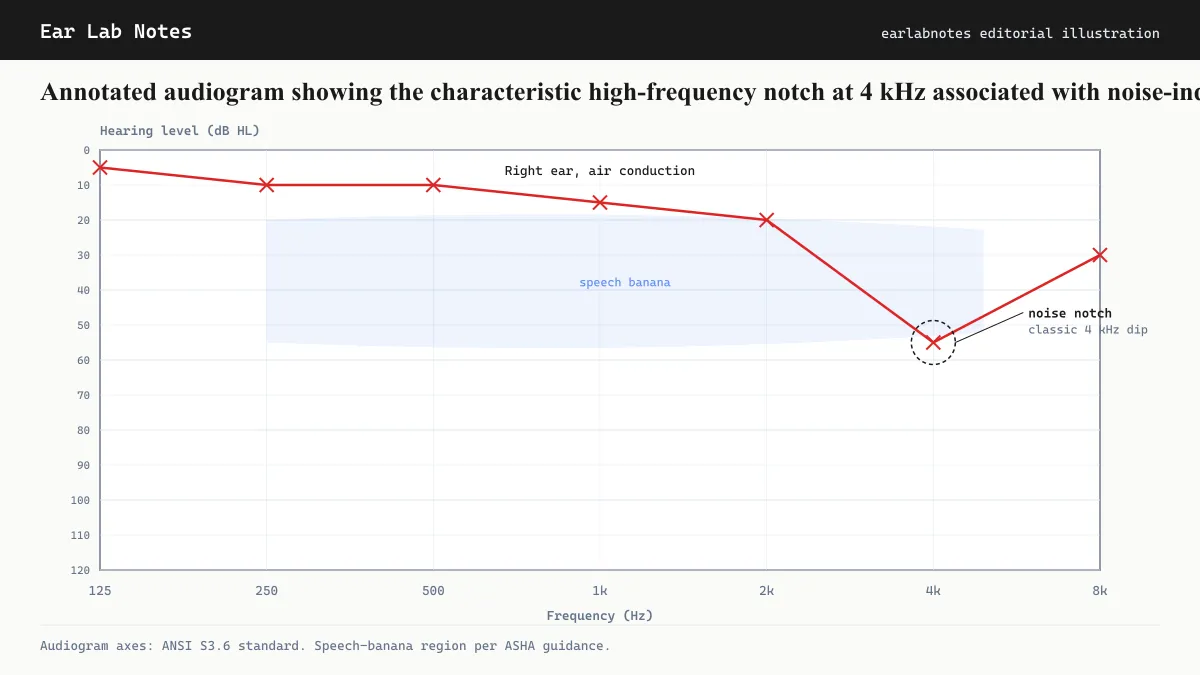
The result is the characteristic audiometric “noise notch”: a dip in hearing thresholds centered around 4 kHz, with better thresholds at adjacent frequencies, that is the hallmark of noise-induced cochlear damage.
Why the tinnitus pitch matches the notch
The central-gain model of tinnitus proposes that when hair cells at a specific cochlear location are damaged or lost, the auditory neurons in that frequency region lose their normal input. These neurons may then increase their spontaneous firing rate, and the brain interprets that activity as sound from that frequency.
The edge effect, a well-documented observation in tinnitus research, refines this further. Tinnitus pitch tends to cluster at or just above the edge of the frequency-loss region, where the contrast between normal and depleted neural input is steepest. This means that a noise notch at 4 kHz will often produce a tinnitus pitch in the 4 to 6 kHz range.
Aging and the spread above 6 kHz
Age-related hearing loss (presbycusis) follows a different but overlapping pattern. Rather than a notch, it tends to produce a gradual slope of increasing loss at higher frequencies, beginning above 4 kHz and extending upward. By the time this loss becomes noticeable to a patient, thresholds above 6 and 8 kHz may be significantly affected.
In practice, many older adults with tinnitus have a combined pattern: a noise notch at 4 kHz from earlier years of noise exposure, sitting on top of a sloping high-frequency loss from aging. This produces a complex tinnitus picture where the perceived pitch may be difficult to attribute cleanly to one cause.
The Mayo Clinic notes that presbycusis is among the most common causes of hearing loss and tinnitus in adults over 60, reflecting the cumulative effect of cochlear hair cell loss over a lifetime.
High-frequency tinnitus and speech comprehension
One of the confusing aspects of high-frequency tinnitus is that it can be present and significant even when speech comprehension seems normal in quiet environments.
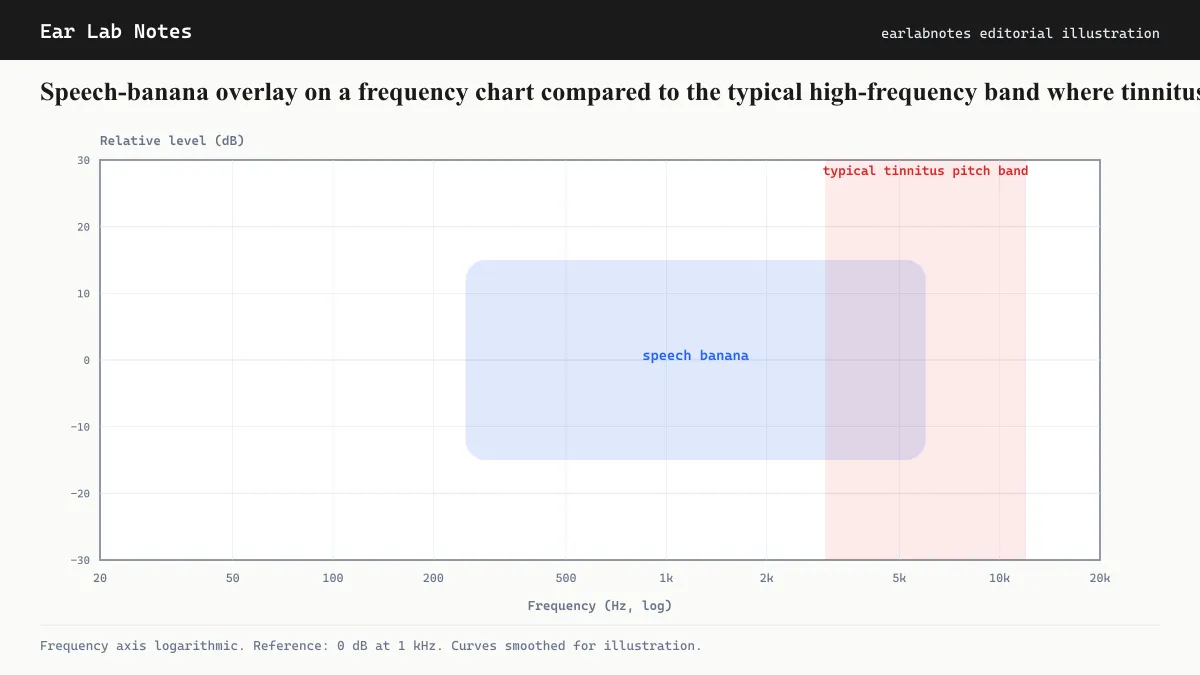
The speech banana, the frequency and volume range within which the sounds of conversational speech fall, occupies roughly 250 Hz to 4,000 Hz. High-frequency tinnitus above this range can be caused by hearing loss that sits above the speech banana, meaning that speech intelligibility is preserved even as the affected cochlear region produces phantom sound.
This explains why many patients report good speech comprehension alongside persistent high-pitched ringing. It also means that tinnitus is sometimes the first noticeable sign of cochlear damage that a standard audiogram might classify as mild or even subclinical at lower frequencies.
Noise exposure and prevention
High-frequency tinnitus caused by noise exposure reflects preventable cochlear damage. NIOSH guidelines specify permissible exposure times at various decibel levels: 8 hours at 85 dB-A, 4 hours at 88 dB-A, 2 hours at 91 dB-A, halving at every 3 dB increase. Sound levels at concerts, nightclubs, and through earbuds at high volume can reach 100 dB-A or more, far exceeding safe exposure durations.
Hearing protection (foam earplugs or earmuffs that achieve sufficient attenuation) can substantially reduce the noise dose at the cochlear level. The NIDCD notes that once cochlear hair cells are damaged, they do not regenerate in humans. Prevention remains the most effective approach to avoiding noise-induced high-frequency tinnitus.
Extended high-frequency audiometry
Standard clinical audiograms test hearing thresholds from 250 Hz to 8,000 Hz. For patients with high-frequency tinnitus whose standard audiogram appears relatively normal, some audiologists offer extended high-frequency testing, which measures thresholds from 8,000 Hz to 16,000 Hz.
Early noise damage often appears first in this extended range before descending into the standard audiogram frequencies. Extended high-frequency audiometry is not universally available but may be informative for younger patients with apparent high-frequency tinnitus and a clean standard audiogram.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- Why does noise damage hit 4 kHz before other frequencies?
- The 4 kHz region of the cochlea sits near the base of the coiled structure, where the traveling wave created by incoming sound creates mechanical stress. Anatomical factors mean this region experiences the most intense vibration for sounds in the midrange, making its hair cells particularly vulnerable to acoustic overexposure. NIOSH and NIDCD both document the 4 kHz notch as the signature pattern of noise-induced cochlear damage.
- Can high-frequency tinnitus go away?
- Acute high-frequency tinnitus after a single loud-noise event often resolves within hours to days. If it has been present for weeks or months, it is much less likely to resolve spontaneously. Habituation, where the brain's response to the signal reduces over time, is achievable for many people, but this is different from the sound disappearing. Consult an audiologist for a realistic assessment of your situation.
- I can hear speech fine but have high-pitched ringing. Is that normal?
- Yes. High-frequency tinnitus often sits above the speech banana (the frequency range of conversational speech). Because speech intelligibility depends mainly on frequencies from about 500 Hz to 4000 Hz, hearing loss and tinnitus that begin above this range can be significant without immediately affecting speech comprehension. A full audiogram will reveal whether high-frequency thresholds have shifted.
- Does high-frequency hearing loss always cause tinnitus?
- No. Many people with high-frequency hearing loss on an audiogram do not experience tinnitus. The mechanism that generates tinnitus, thought to involve compensatory changes in central auditory gain, does not develop in everyone with the same cochlear damage. The reasons for this variability are not fully understood.
Primary sources
Where this comes from
- ◆ Noise-induced Hearing Loss · NIH/NIDCD
- ◆ Permissible Noise Exposures · NIOSH/CDC
- ◆ Tinnitus · NIH/NIDCD
- ◆ Hearing Loss · Mayo Clinic
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N014 · The Ear Lab · earlabs.app