The principle behind masking
Before considering the devices, it helps to understand the acoustic principle they apply.
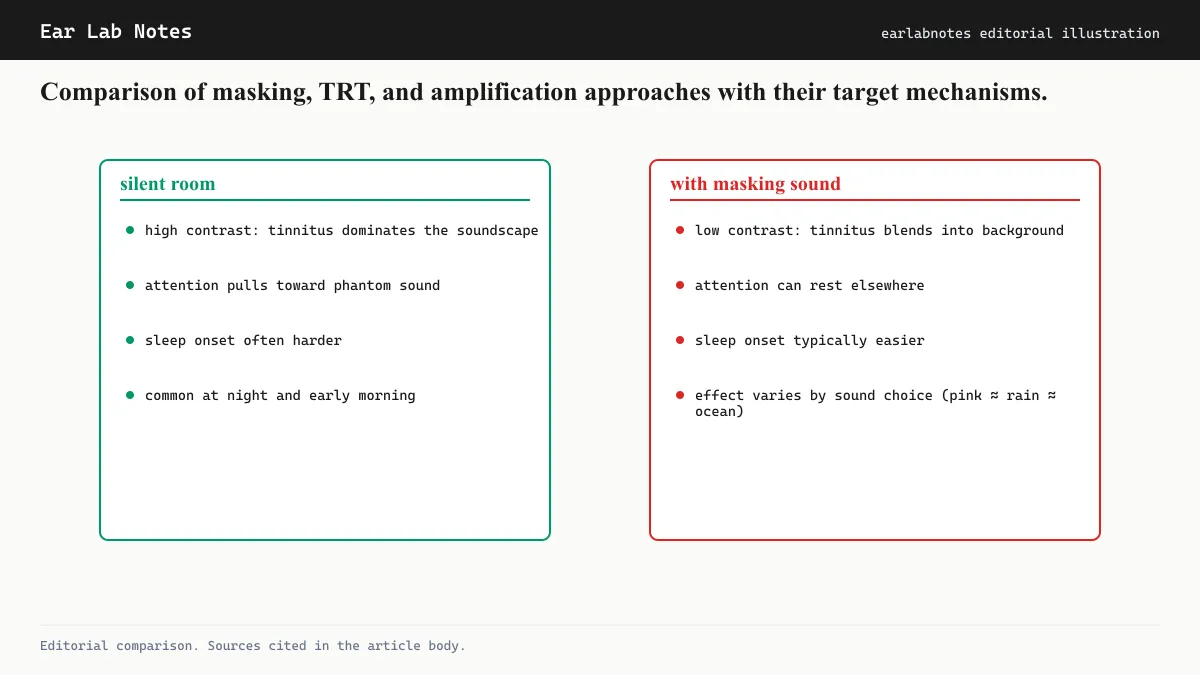
Tinnitus is most noticeable when the surrounding environment is quiet. The phantom sound that exists only inside the auditory nervous system has no competition in silence, and the brain has no difficulty attending to it.
Masking introduces a real acoustic signal that partially overlaps with the frequency range of the tinnitus. The auditory system, which can only process a finite amount of information simultaneously, perceives both signals but with reduced contrast between them. Tinnitus becomes less salient, similar to the way a conversation at a party becomes harder to follow when competing conversations begin nearby.
The degree of masking depends on the spectral overlap between the masking sound and the tinnitus pitch, the relative loudness of each, and the individual’s auditory system characteristics.
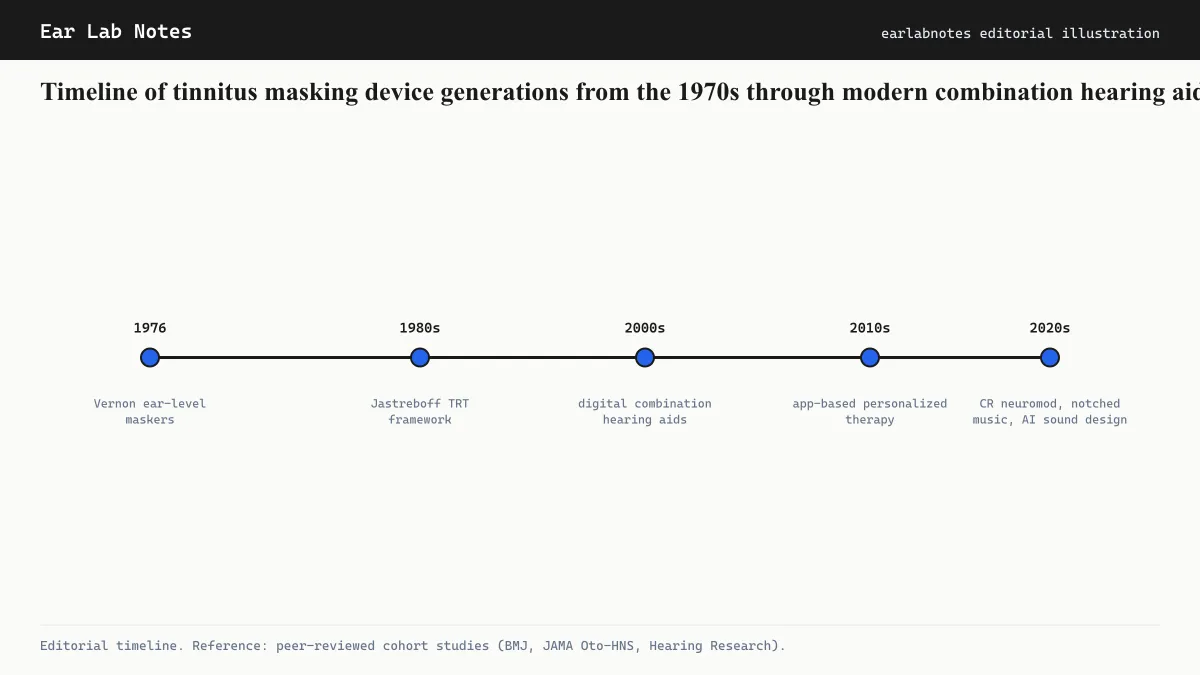
Early masking devices
Formal use of wearable sound generators for tinnitus dates to the 1970s, when clinical researchers began experimenting with earpieces that produced white noise or narrowband noise. These early devices were analog, fixed in their sound output, and worn behind or in the ear.
Their limitations were significant. They could not be adjusted for individual tinnitus pitch. They had limited battery life and basic acoustic quality. Because they only masked and did not amplify, they were of little use to the large proportion of tinnitus patients who also had hearing loss.
Nonetheless, they established a clinical rationale that remains valid: delivering a low-level broadband sound to the ear reduces the perceptual prominence of tinnitus.
Digital sound generators
Digital sound generation allowed considerably more flexibility. Clinically fitted sound generators of the 1990s and 2000s could be programmed to adjust spectral shape, to some extent matching the output to the patient’s tinnitus pitch, and to set precise output levels.
They remained dedicated masking devices without amplification. Fitting required audiological assessment, and the goal was to find a level of masking sound that reduced tinnitus prominence without being intrusive or fatiguing in itself.
An important refinement came with the development of tinnitus retraining therapy in the late 1980s and 1990s. The TRT protocol uses sound generators at a lower level than traditional masking, aiming not to mask the tinnitus completely but to provide a background that makes the tinnitus less prominent. The theory is that partial masking, combined with structured counseling, promotes habituation more effectively than complete masking, which may delay it.
Combination hearing aids
The most clinically significant development for tinnitus masking technology has been the integration of sound generators into hearing aids. Combination devices serve two purposes simultaneously: they amplify external sound to compensate for hearing loss, and they deliver a configurable masking or sound enrichment signal through the same earpiece.
This matters because the majority of people seeking clinical care for tinnitus have some degree of hearing loss. In these cases, hearing aid amplification alone often reduces perceived tinnitus prominence by increasing the level of environmental sound, which provides natural masking. Adding a built-in sound generator allows further customization for cases where amplification alone is insufficient.
Modern combination devices are fully digital, programmable through audiological software, and offer a range of sound options including white noise, pink noise, brown noise, and nature-inspired sounds. They can also modulate the masking level automatically based on the ambient environment.
The AAO-HNS clinical practice guideline for tinnitus recommends that clinicians discuss sound therapy options with patients and notes that combination devices are a recognized approach for people with concurrent hearing loss.
What masking cannot do
It is important to be clear about the limits of masking devices, including combination aids.
No masking device treats tinnitus at its source. The phantom signal continues to be generated within the auditory nervous system. When the device is removed, tinnitus returns to its prior level.
Masking alone is generally considered insufficient as a standalone treatment for significant tinnitus distress. The AAO-HNS guideline and guidance from the British Tinnitus Association both emphasize that sound therapy is most effective when combined with counseling and, in appropriate cases, psychological interventions such as CBT.
Volume management remains important. A masking device operated at an inappropriate level over long periods could theoretically contribute to the noise exposure it is meant to help with. Proper fitting by an audiologist includes verifying that output levels are within safe ranges.
The minimum masking level concept
A clinical concept specific to masking devices is the minimum masking level (MML), the lowest volume at which a given sound completely covers the patient’s tinnitus perception. MML is measured during fitting and serves as a guide to the output level at which the device operates.
Devices are typically programmed to operate below MML, particularly in TRT protocols, where partial masking rather than complete masking is the target. Operating at or above MML suppresses tinnitus awareness but may slow the habituation process by removing the signal the brain needs to practice ignoring. Operating below MML provides acoustic enrichment while still allowing some tinnitus perception.
This nuance is one reason self-management with a consumer device may be less effective than audiologist-fitted management. Without MML measurement, there is no calibrated target for the masking level.
The evidence base for masking devices
Published studies on dedicated masking devices and combination hearing aids for tinnitus show generally positive results for subjective tinnitus handicap scores, though trial quality varies. The AAO-HNS clinical practice guideline notes that evidence for sound therapy as a component of tinnitus management is positive overall, while acknowledging that more high-quality randomized trials are needed.
Combination devices that address both hearing loss and tinnitus have a particularly consistent evidence base, because hearing aid amplification alone reduces tinnitus salience by enriching the acoustic environment. Adding a built-in masker provides an additional tool when amplification alone is insufficient.
How devices are fitted and accessed
In clinical practice, masking devices and combination hearing aids are fitted by audiologists following a full audiological assessment. This typically includes a pure-tone audiogram, tinnitus pitch matching, loudness matching, and assessment of minimum masking level, all of which inform the appropriate device characteristics and settings.
Access in the United Kingdom is available through the NHS, where audiologists in ENT departments or hearing services can assess and provide devices for appropriate patients. The British Tinnitus Association also maintains guidance on what to expect from sound-device assessment, which can help patients know what to ask for. In other countries, private audiology practices and in some cases specialist tinnitus clinics are the primary access points.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- What does a tinnitus masking device do?
- A masking device generates a broadband sound, typically white or pink noise, delivered through an earpiece. The sound partially fills the auditory frequency channels occupied by tinnitus, reducing the contrast between the phantom sound and the background. This makes tinnitus less perceptible while the device is in use.
- Is a masking device the same as a hearing aid?
- Not exactly. A hearing aid amplifies external sounds to compensate for hearing loss. A dedicated masking device generates sound rather than amplifying it. A combination device does both: it provides hearing aid amplification and also contains a built-in sound generator for masking. Combination devices are now common in audiology practice.
- How is a masking device different from sound enrichment at home?
- A wearable masking device delivers sound directly to the ear, providing consistent masking wherever the person goes. Home sound enrichment, through speakers or noise machines, is limited to specific rooms. For people whose tinnitus is disruptive throughout the day in varied environments, a wearable device offers more consistent coverage.
- Do masking devices treat tinnitus permanently?
- No masking device treats or eliminates tinnitus. The masking effect is present only when the device is in use. Some clinicians and researchers have proposed that habituation may carry over beyond active masking periods when devices are used as part of a structured program, but this is not established as a reliable outcome from masking alone.
- Who prescribes tinnitus masking devices?
- Audiologists are the primary clinical professionals who assess, fit, and program tinnitus masking devices and combination hearing aids. Referral typically comes from a GP or ENT specialist after a clinical evaluation of tinnitus.
Primary sources
Where this comes from
- ◆ Tinnitus: Assessment and Management · NIH/NIDCD
- ◆ Tinnitus Clinical Practice Guideline · AAO-HNS
- ◆ Tinnitus sound therapy · British Tinnitus Association
- ◆ Tinnitus: Diagnosis and treatment · Mayo Clinic
- ◆ Tinnitus overview · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N020 · The Ear Lab · earlabs.app