Meniere’s disease is a disorder of the inner ear that produces episodic attacks combining four core features: vertigo, fluctuating hearing loss, a sensation of pressure or fullness in the ear, and tinnitus. NIDCD estimates that about 615,000 people in the United States have Meniere’s disease, with approximately 45,500 new cases diagnosed annually.
The tinnitus of Meniere’s disease has a distinctive character that separates it from noise-induced ringing. Understanding this distinction helps clinicians identify the condition and helps people with the disorder interpret what they are experiencing.
The Meniere’s triad and why tinnitus fits differently
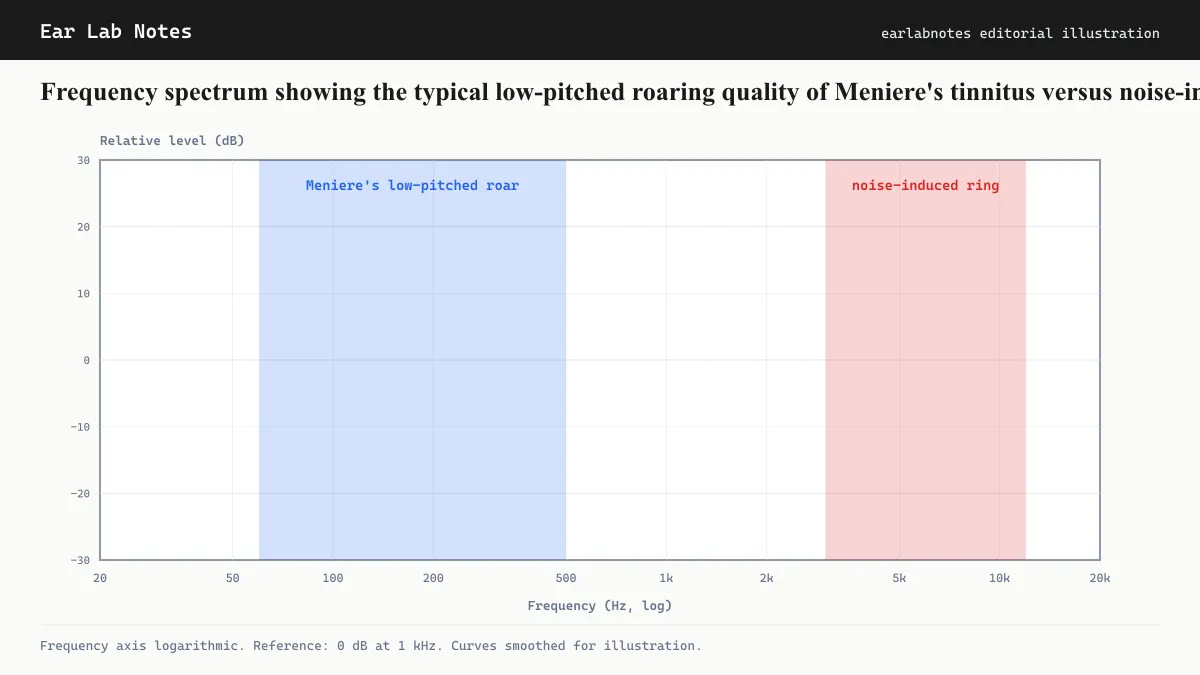
The diagnostic criteria for Meniere’s disease require at least two spontaneous episodes of vertigo lasting 20 minutes to 12 hours, audiometrically documented low-to-mid frequency hearing loss in the affected ear on at least one occasion, and fluctuating hearing or tinnitus in that ear. Tinnitus in this context is typically described as a low-pitched roaring, buzzing, or rushing sound rather than the high-pitched ringing associated with noise or aging.
The low-frequency character reflects the underlying pathology. Noise damages the high-frequency region of the cochlea (the base). Meniere’s disease affects the low-frequency region (the apex) first and most prominently, particularly in early stages.
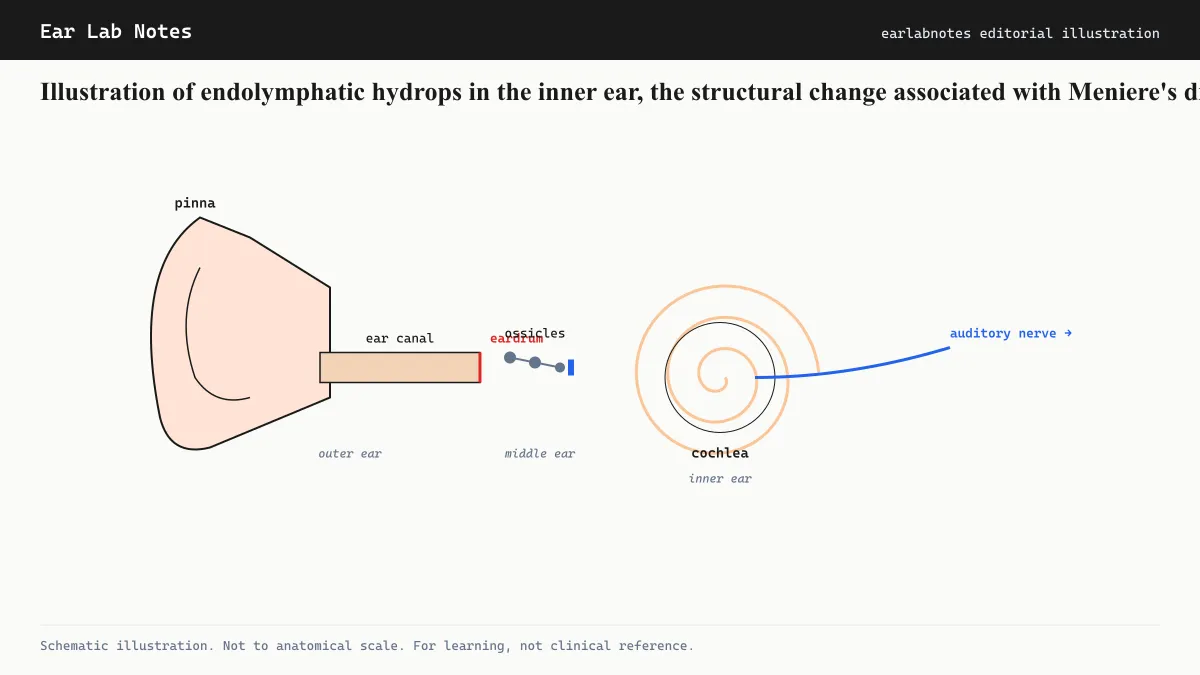
Endolymphatic hydrops: the structural finding
The structural change associated with Meniere’s disease is endolymphatic hydrops, an abnormal expansion of the endolymphatic compartment of the inner ear. The inner ear contains two fluid systems: endolymph (high potassium, low sodium, filling the membranous labyrinth) and perilymph (high sodium, surrounding the membranous labyrinth). These compartments are normally maintained at specific volumes and compositions.
In Meniere’s disease, endolymph volume increases, distending the membranous labyrinth. This distension is thought to disrupt the mechanoelectrical function of hair cells (impairing hearing) and the fluid dynamics of the semicircular canals (producing vertigo). Tinnitus arises as a consequence of this disruption to normal cochlear signaling.
What causes the endolymph overaccumulation is not definitively established. Leading hypotheses involve abnormal production or absorption of endolymph, possibly linked to genetic predisposition, autoimmune factors, viral injury to the endolymphatic sac (the structure responsible for endolymph regulation), or vascular factors. The condition is not contagious and is not caused by lifestyle factors in any simple sense, though triggers and modulators exist.
How Meniere’s tinnitus fluctuates
A hallmark of Meniere’s tinnitus, in contrast to most other forms, is that it fluctuates markedly in intensity. Many people with the condition report that tinnitus worsens in the hours or minutes before an attack of vertigo, serving as a warning signal. During the attack, the tinnitus can intensify substantially. After the attack resolves, tinnitus often, though not always, reduces.
Over time, as the disease progresses and cumulative cochlear damage accumulates, the hearing loss and tinnitus may become more constant and less tied to the episodic attack pattern. Late-stage Meniere’s disease can resemble noise-induced cochlear damage audiometrically, which is one reason early evaluation and documentation are important.
How Meniere’s tinnitus differs from noise-induced tinnitus
The table below summarizes key distinguishing features:
| Feature | Meniere’s tinnitus | Noise-induced tinnitus |
|---|---|---|
| Pitch | Low-frequency (roaring, buzzing) | High-frequency (ringing, hissing) |
| Onset | Episodic, tied to attacks | Often gradual after cumulative exposure |
| Fluctuation | Marked fluctuation over days/weeks | Relatively stable day to day |
| Associated symptoms | Vertigo, ear fullness, hearing fluctuation | Hearing loss (often high-frequency), no vertigo |
| Audiogram pattern | Low-frequency hearing loss (early stages) | Noise notch at 4 kHz |
Standard management approaches
AAO-HNS guidelines on Meniere’s disease address management of all four symptoms, including tinnitus. The management hierarchy moves from conservative to more invasive:
Dietary modification: Low-sodium diet (typically 1,500 to 2,000 mg per day) and fluid balance management are first-line recommendations because reducing sodium intake is thought to reduce endolymph volume. Evidence is largely observational but supports this approach in many patients.
Diuretics: Thiazide or loop diuretics are sometimes prescribed alongside dietary sodium restriction to reduce fluid retention, on the same rationale.
Vestibular rehabilitation: For balance-related disability between attacks, vestibular physical therapy can improve functional stability.
Transtympanic treatments: For people who do not respond to conservative management, injection of corticosteroids or gentamicin into the middle ear through the tympanic membrane is a recognized escalation. Gentamicin reduces vestibular function in the treated ear, substantially reducing vertigo attacks. This approach carries a risk of further hearing loss in the treated ear and is not used lightly.
Surgical options: For severe, refractory cases, endolymphatic sac procedures or labyrinthectomy may be considered. These carry significant implications for hearing and balance function.
For the tinnitus specifically, the approaches used for other forms (sound therapy, cognitive behavioral therapy) remain applicable alongside disease-specific management.
Living with Meniere’s tinnitus
The unpredictability of Meniere’s disease, the sudden vertigo attacks, the fluctuating hearing, and the variable tinnitus intensity, creates a distinctive psychological burden. Organizations including NIDCD and the Vestibular Disorders Association provide educational resources for people learning to manage the condition day to day.
A neurotologist (an otolaryngologist with specialized vestibular training) is the most appropriate specialist for complex Meniere’s cases, while an audiologist monitors hearing function and provides rehabilitation for hearing and tinnitus-related aspects.
The psychological dimension
The episodic and unpredictable nature of Meniere’s disease creates a distinctive form of anxiety that is rarely seen in other tinnitus conditions. A person with noise-induced tinnitus typically experiences a relatively stable signal they can learn to habituate to. A person with Meniere’s never knows when the next violent episode of vertigo will arrive, which creates hypervigilance around even minor changes in tinnitus quality or ear fullness.
This anxiety about the next attack is itself a recognized contributor to disability in Meniere’s disease and is not a character failing. Cognitive behavioral therapy and mindfulness-based approaches, the same tools used for other tinnitus types, have been studied in Meniere’s populations and may help reduce the anticipatory anxiety that compounds distress between attacks. Support groups, including those connected to vestibular disorder organizations, can also provide perspective from others managing the same day-to-day uncertainty.
Tracking symptoms over time
Maintaining a diary of attack frequency, duration, associated tinnitus intensity, and potential triggers is recommended by many clinical programs for Meniere’s disease. This record serves two purposes: it provides data the clinical team can use to assess whether treatment is stabilizing the condition, and it helps identify individual-level triggers that may be modifiable. Tinnitus fluctuation often tracks closely with overall disease activity, making the diary useful for both components.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- Is Meniere's disease the only condition that causes low-pitched tinnitus?
- No. Low-pitched tinnitus can also result from eustachian tube dysfunction, superior semicircular canal dehiscence, and some vascular conditions. However, Meniere's disease is among the most common identifiable causes of low-pitched roaring tinnitus when accompanied by vertigo and fluctuating hearing loss. Diagnosis requires clinical evaluation.
- Does a low-sodium diet always help Meniere's tinnitus?
- Low-sodium diet is a standard first-line recommendation for Meniere's disease management per AAO-HNS guidance, based on the role of sodium in regulating endolymph volume. However, response to dietary modification varies between individuals and the evidence base for this specific recommendation relies substantially on observational data rather than large randomized trials.
- Can Meniere's disease affect both ears?
- Meniere's disease most commonly begins in one ear (unilateral). Over time, bilateral involvement occurs in a meaningful proportion of people, though estimates of this proportion vary considerably across studies. An otolaryngologist or neurotologist experienced in vestibular disorders can monitor for bilateral progression.
- What triggers a Meniere's attack?
- Reported triggers include high sodium intake, caffeine, stress, alcohol, and barometric pressure changes, though the evidence for specific triggers is largely observational and varies between individuals. Identifying personal triggers through a symptom diary is often part of the self-management approach recommended alongside medical treatment.
Primary sources
Where this comes from
- ◆ Meniere's Disease - NIDCD · National Institute on Deafness and Other Communication Disorders
- ◆ Meniere's Disease - Mayo Clinic · Mayo Clinic
- ◆ Clinical Practice Guideline: Meniere's Disease - AAO-HNS · American Academy of Otolaryngology, Head and Neck Surgery
- ◆ Meniere's Disease - NHS · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N021 · The Ear Lab · earlabs.app