Pulsatile tinnitus is a form of tinnitus in which the perceived sound beats in synchrony with the heartbeat. People describe it as a whooshing, thumping, rushing, or drumming sound inside or behind the ear, timed to their pulse. It is mechanically distinct from the continuous ringing or hissing of ordinary (non-pulsatile) tinnitus: where ordinary tinnitus is generated by the auditory nervous system in the absence of any physical sound, pulsatile tinnitus typically arises from an actual acoustic source inside the body, most commonly turbulent blood flow transmitted through bone and tissue to the cochlea.
This mechanical distinction makes pulsatile tinnitus clinically important. Some of its causes are benign; others are vascular or structural conditions that benefit from specific treatment and that imaging can identify.
Why blood flow can become audible
Under normal physiological conditions, blood moves through vessels in smooth laminar flow that generates no sound perceptible to the cochlea. Several conditions disrupt this and create turbulence or increased flow:
Elevated blood pressure: Higher cardiac output forces blood through vessels with greater velocity and turbulence. When this occurs in vessels near the ear, such as the internal carotid artery or the jugular vein, the sound energy generated can be transmitted to the cochlea.
Venous hum: The jugular veins carry blood back toward the heart on both sides of the neck. A high-riding or dehiscent (exposed) jugular bulb sits immediately beneath the floor of the middle ear. In some people, particularly during states of increased cardiac output such as pregnancy, anemia, or hyperthyroidism, the venous flow becomes turbulent enough to generate a hum audible to the cochlea. This is one of the more common and generally benign causes of pulsatile tinnitus.
Atherosclerotic stenosis: Narrowing of the carotid or vertebral arteries from plaque deposits creates a focal high-velocity jet that generates turbulent sound. The sound of flow through a narrowed vessel is called a bruit.
Arteriovenous malformations (AVMs) and fistulae: Abnormal direct connections between arteries and veins, bypassing the normal capillary network, create high-velocity, high-turbulence flow. Dural arteriovenous fistulae (DAVFs), occurring in the tissue covering the brain near the ear, are a recognized cause of pulsatile tinnitus. They can also cause other neurological symptoms and often require specialist management.
Idiopathic intracranial hypertension (IIH): Elevated pressure in the cerebrospinal fluid surrounding the brain transmits to the venous sinuses and can produce audible venous flow, typically louder when lying down. IIH is associated with headache and visual changes in addition to tinnitus, and occurs more commonly in women of reproductive age with obesity.
Glomus tumors: These rare, highly vascular tumors can arise in the jugular foramen or middle ear (glomus jugulare, glomus tympanicum) and produce pulsatile tinnitus by placing a vascular mass directly adjacent to the middle ear structures. They may also be associated with a visible reddish mass behind the eardrum on examination.
The anatomy that makes this possible
The inner ear sits within the petrous portion of the temporal bone, a dense, compact structure that also contains the internal carotid artery in its own canal (the carotid canal), and houses the sigmoid sinus and jugular bulb nearby. This tight anatomical clustering means that turbulence in any of these structures is acoustically coupled to the cochlea through bone conduction.
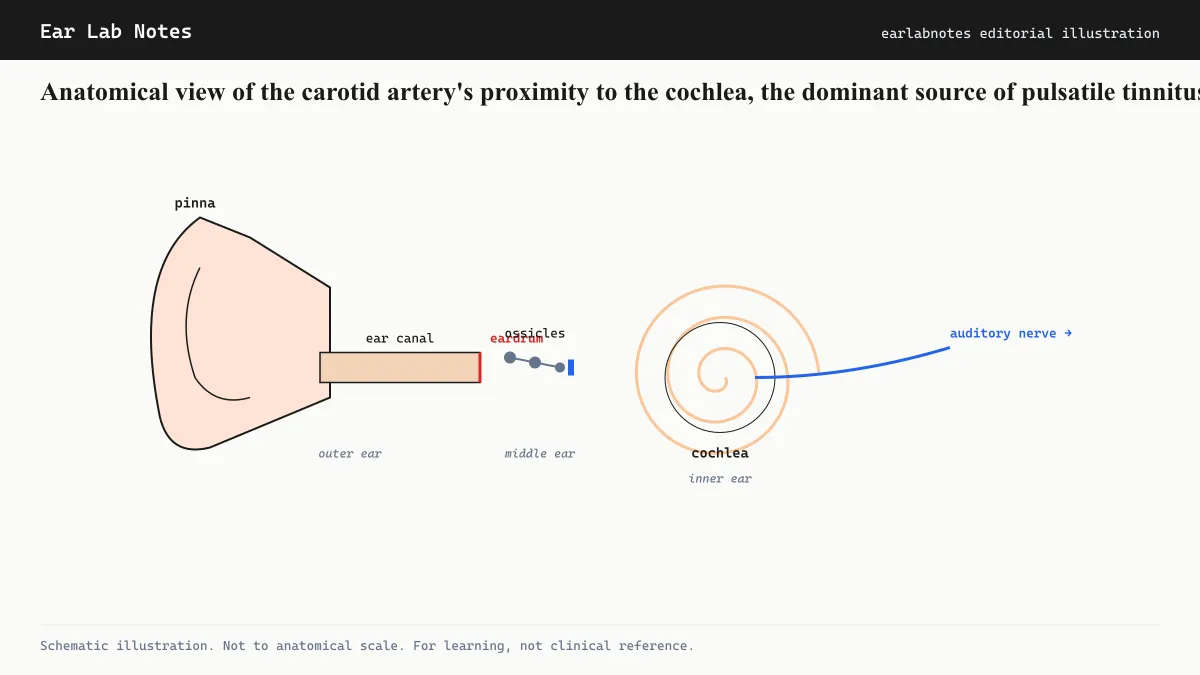
The proximity is so close that, in cases of aberrant internal carotid artery (a congenital variant where the artery takes an unusual course directly through the middle ear), people may see a pulsating reddish structure through their eardrum on otoscopic examination, and the pulsatile sound may be audible to the examining clinician.
How pulsatile tinnitus presents
The defining perceptual feature is synchrony with the heartbeat. Most people notice it most acutely in quiet environments, particularly at night when external sound is minimal. Some note that the thumping sound speeds up with exercise and slows with rest, tracking the cardiac rate. Others find that turning their head or changing position briefly alters the intensity.
A practical clinical test: pressing firmly on the ipsilateral (same-side) jugular vein while attending to the tinnitus. If pressure reduces the sound, this suggests a venous source, a clinically useful finding that narrows the differential.
Clinical evaluation
AAO-HNS guidance and Mayo Clinic both recommend evaluation of pulsatile tinnitus that includes imaging in most cases. The typical workup includes:
-
Medical history and physical examination, including blood pressure measurement and auscultation of the neck, mastoid region, and periauricular area for bruits.
-
Pure-tone audiogram to assess cochlear hearing function and whether sensorineural hearing loss coexists.
-
CT of the temporal bone (without contrast) to evaluate bony structures including the carotid canal, jugular bulb, and tegmen for anatomical variants or dehiscence.
-
CT angiography or MR angiography of the head and neck if vascular causes such as stenosis, AVM, or DAVF are suspected.
-
Ophthalmological evaluation if IIH is on the differential, to assess for papilledema (optic nerve swelling from elevated CSF pressure).
The evaluation is guided by the history: whether the tinnitus is unilateral or bilateral, whether it changes with position or compression, and whether other symptoms (headache, visual changes, pulsatile sensation in the head) are present.
When pulsatile tinnitus can be treated at the source
Unlike most subjective tinnitus, some pulsatile forms have directly addressable causes:
- Blood pressure control can reduce flow-related turbulence in hypertension-driven cases.
- Weight loss and CSF pressure-lowering treatment can improve IIH-related pulsatile tinnitus.
- Endovascular embolization or stereotactic radiosurgery can treat DAVFs.
- Surgical options exist for symptomatic glomus tumors.
- In some cases of sigmoid sinus dehiscence, surgical repair of the bony defect can reduce or eliminate pulsatile tinnitus.
These targeted treatments are relevant only when the specific cause has been identified through imaging. Applying audiological management tools (sound therapy, CBT) without first excluding a treatable vascular cause in pulsatile tinnitus is considered suboptimal clinical practice.
When pulsatile tinnitus is benign
Many cases of pulsatile tinnitus, after thorough evaluation, turn out to have no structurally dangerous cause. Benign venous hum, heightened awareness of normal carotid flow during periods of anxiety or hypervigilance, and mild anatomical variants that do not require intervention account for a significant proportion of evaluated cases. For these individuals, the same management tools used for non-pulsatile subjective tinnitus are applicable.
The important goal of evaluation is not to create anxiety, but to ensure that the minority of cases with treatable structural causes are identified and managed appropriately.
If symptoms persist or change, see an audiologist or physician.
Related notes
Watch
Pulsatile Tinnitus, with Dr. Joseph Breen
Source: Mayo Clinic on YouTube
Transcript / summary
Frequently asked
Questions readers ask
- Is pulsatile tinnitus always a sign of something serious?
- Not always. Many cases of pulsatile tinnitus result from benign causes such as increased blood flow during exercise, anemia, or temporary sinus congestion. However, a meaningful subset have vascular or structural causes that benefit from specific treatment and that should not be missed. This is why clinicians recommend evaluation and often imaging for new pulsatile tinnitus.
- Can I test at home whether my tinnitus is pulsatile?
- You can check whether the sound rhythmically matches your heartbeat by pressing gently on your wrist to find your pulse while listening to the tinnitus. If the rhythm aligns, it is consistent with pulsatile tinnitus. This is useful information to bring to a clinical evaluation, but it does not replace formal assessment. Some people with pulsatile tinnitus find the rhythm easier to detect when lying quietly on their side.
- Will pulsatile tinnitus get louder over time?
- This depends entirely on the underlying cause. Pulsatile tinnitus from benign venous hum or mild hypertension may remain stable or improve with blood pressure management. Tinnitus from a progressive vascular lesion could worsen. Regular follow-up with a clinician familiar with the cause is the appropriate way to monitor any change.
- What imaging is used to investigate pulsatile tinnitus?
- Typical imaging options include CT angiography (CTA) or MRI with MR angiography (MRA) of the head and neck to visualize vascular structures. The specific protocol is chosen based on the suspected cause. CT of the temporal bone without contrast can identify bony abnormalities such as dehiscence of the jugular bulb or aberrant carotid canal. A clinician or neuroradiologist will select the most appropriate modality.
- My pulsatile tinnitus goes away when I press on my neck. Is that significant?
- Yes, this is a clinically relevant finding known as the compression test. Pressure on the jugular vein can temporarily reduce venous pulsatile tinnitus because it alters flow dynamics. This finding often suggests a venous rather than arterial source, which helps narrow the differential diagnosis. Report this observation to the evaluating clinician.
Primary sources
Where this comes from
- ◆ Tinnitus - NIDCD · National Institute on Deafness and Other Communication Disorders
- ◆ Tinnitus - Mayo Clinic · Mayo Clinic
- ◆ Clinical Practice Guideline: Tinnitus - AAO-HNS · American Academy of Otolaryngology, Head and Neck Surgery
- ◆ Tinnitus - NHS · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N029 · The Ear Lab · earlabs.app