Most tinnitus originates in the auditory system. A damaged cochlea sends distorted signals, or a deprived auditory brain generates its own internal noise to compensate. But a meaningful subset of tinnitus cases behave differently. They can be modified by physical input: moving the jaw, pressing on a neck muscle, or even shifting the eyes to an extreme position can change the pitch or loudness of the tinnitus.
This category is called somatic or somatosensory tinnitus. Understanding it matters because it points toward a different mechanism, and sometimes a different set of specialists, compared to cochlear or purely central tinnitus.
What makes it somatic
The term somatic (from Greek soma, body) reflects the role of the musculoskeletal system in producing or modulating the tinnitus. Specifically, somatosensory pathways that carry signals from the body, not the ear, appear to feed into the auditory brainstem in a way that can generate or alter the phantom sound.
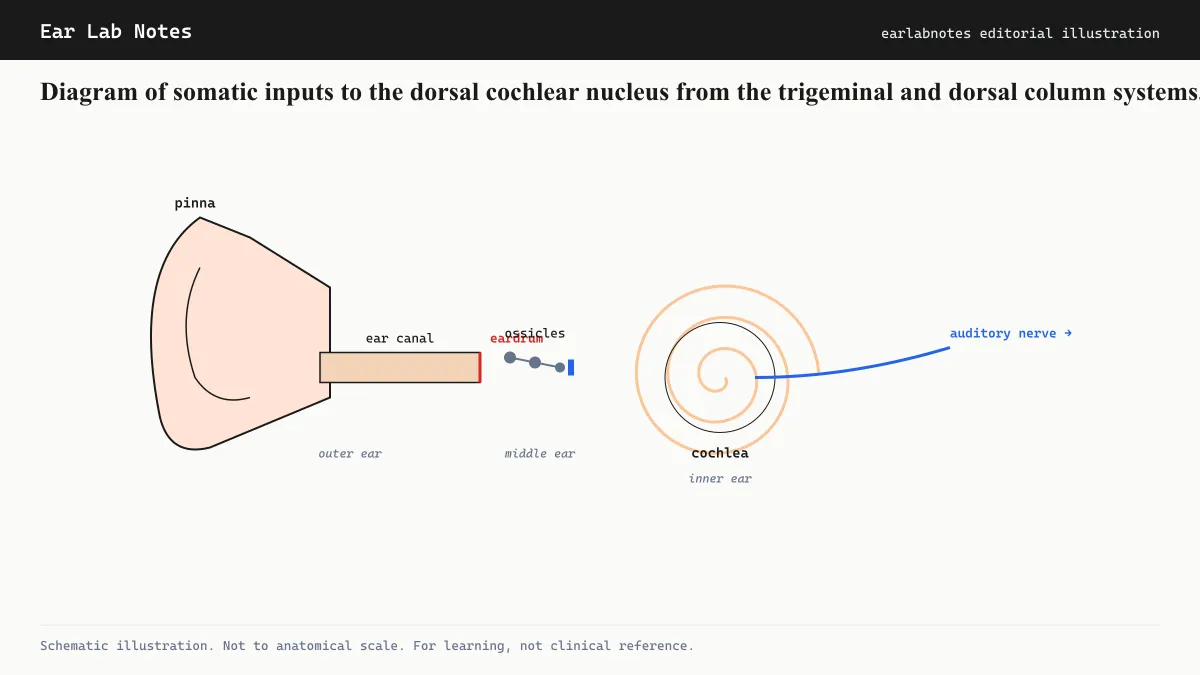
The key anatomical structure is the dorsal cochlear nucleus (DCN). The DCN is an auditory relay station in the brainstem that receives not only the expected auditory signals from the cochlea via the eighth cranial nerve, but also non-auditory input from two somatosensory systems.
The trigeminal nerve (fifth cranial nerve) carries signals from the jaw, face, and upper neck. The dorsal column nuclei carry signals from the body’s proprioceptive and touch sensors, including the cervical spine. Both of these converge on the DCN alongside auditory input.
When the auditory input to the DCN is reduced or distorted, somatosensory inputs may gain disproportionate influence over the DCN’s output, essentially contributing to the phantom signal that becomes tinnitus.
How clinicians test for it
The defining feature of somatic tinnitus is modulability: the tinnitus changes in response to physical maneuvers. Audiologists and otolaryngologists use a set of standardized maneuvers to test this.
Common maneuvers include:
- Pressing firmly on the jaw, temporomandibular joint, or surrounding muscles
- Clenching the teeth
- Turning the head to the left or right while holding it in position
- Pressing on muscles of the upper neck or behind the ear
- Moving the eyes to extreme positions (left, right, up, down)
For each maneuver, the patient reports whether the tinnitus pitch increased, decreased, or changed in quality. A positive result, where one or more maneuvers reliably alter the tinnitus, is consistent with a somatosensory component.
Importantly, some degree of somatosensory modulation is present in a substantial minority of tinnitus patients generally. Estimates in the literature vary widely, with some studies finding modulation in 40 to 80 percent of people with chronic tinnitus. Not all of these represent “somatic tinnitus” in the stricter clinical sense. The term is generally reserved for cases where somatic input appears to be a primary driver, not just a mild modifier.
Common physical sources
TMJ and jaw disorders
The temporomandibular joint (TMJ) is anatomically adjacent to the ear canal and middle ear. The muscles and ligaments involved in jaw movement are served by the trigeminal nerve, which connects directly to the DCN. This is why TMJ disorders are one of the most discussed causes of somatic tinnitus.
Bruxism (tooth grinding), jaw malalignment, and TMJ arthritis can all produce somatic input capable of influencing the auditory brainstem. Tinnitus in this context often fluctuates with jaw tension and may be worse in the morning if bruxism is a factor.
Cervical spine and neck muscles
Cervicogenic tinnitus refers to tinnitus originating from or modulated by the cervical spine, particularly the upper cervical vertebrae and the muscles that attach to them. Injuries such as whiplash, or chronic tension in the sternocleidomastoid and trapezius muscles, can generate somatosensory signals that influence DCN activity.
Patients sometimes notice that their tinnitus changes after periods of sustained neck strain, like long hours at a computer, or that a particular neck position reliably alters the sound.
Eye movement
Some people find that extreme lateral or vertical gaze changes their tinnitus. This suggests involvement of the oculomotor system’s connections to the auditory brainstem, though this is among the less understood aspects of somatosensory modulation.
Why the distinction matters for management
Diagnosing a somatic component has practical implications. If a TMJ disorder is contributing, a dentist or oral maxillofacial specialist may be involved in treatment. If cervical muscle tension is a factor, a physiotherapist with experience in craniocervical conditions may contribute to the management plan.
This does not mean somatic tinnitus is easy to treat. Evidence from controlled trials is limited, and case series show variable outcomes. But identifying the somatosensory contribution can:
- Direct evaluation toward the appropriate specialist
- Avoid unnecessary audiological investigations when a musculoskeletal cause is primary
- Open a management pathway (physical therapy, dental treatment) that would not be considered for standard cochlear tinnitus
For patients with concurrent hearing loss and somatic features, the management typically addresses both the auditory and musculoskeletal components simultaneously.
Somatic tinnitus and the broader tinnitus picture
Somatic tinnitus is not a separate disease. It is a presentation subtype of tinnitus, defined by its modifiability and its mechanism. Most people with somatic tinnitus also have some degree of cochlear involvement or central auditory reorganization.
The BTA and NIDCD both note that tinnitus classification can be useful for directing care, but that many patients fall along a spectrum rather than neatly into one category. A thorough audiological evaluation is the appropriate starting point, from which the presence of somatosensory features can be formally assessed.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- How do I know if my tinnitus is somatic?
- A key sign is that your tinnitus pitch or loudness changes when you move your jaw, press on your neck muscles, clench your teeth, or move your eyes to an extreme position. This is called somatosensory modulation and is the basis for clinical testing. A formal assessment by an audiologist or otolaryngologist is needed to confirm somatic tinnitus and rule out other causes.
- Is somatic tinnitus easier to treat than other types?
- Some clinicians consider somatic tinnitus more amenable to management because it often has a musculoskeletal component that physical therapists or dentists can address. However, evidence is still emerging, and outcomes vary considerably. The diagnostic distinction is most useful for directing evaluation toward the appropriate specialist team.
- Can a neck injury cause tinnitus?
- Cervicogenic (neck-related) tinnitus is a recognized subtype of somatic tinnitus. Injuries to the upper cervical spine can influence the dorsal cochlear nucleus through somatosensory pathways. Assessment by both an audiologist and a musculoskeletal specialist is typically recommended when a temporal relationship between a neck injury and new tinnitus is present.
- Does somatic tinnitus go away if the underlying physical cause is treated?
- In some cases, addressing the underlying musculoskeletal issue (TMJ disorder, cervical muscle tension) reduces or eliminates the tinnitus. But this is not guaranteed, and the evidence is largely from observational studies and case series rather than large controlled trials. Consult both an audiologist and the relevant specialist for realistic expectations.
Primary sources
Where this comes from
- ◆ Tinnitus · NIH/NIDCD
- ◆ Clinical Practice Guideline: Tinnitus · American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- ◆ Tinnitus: causes and management · NHS UK
- ◆ Somatic Tinnitus · British Tinnitus Association (BTA)
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N033 · The Ear Lab · earlabs.app