Tinnitus is among the most commonly reported symptoms following head injury, occurring in studies of both civilian and military populations at rates well above the general population. What makes post-traumatic tinnitus clinically distinct is that it can appear, or persist, even when a standard audiogram shows normal hearing thresholds. This observation points to disruption in the central auditory pathway rather than, or in addition to, peripheral cochlear damage.
How head injury affects the auditory system
A traumatic brain injury (TBI) does not need to be severe to produce tinnitus. Mild TBI, which includes most concussions, is sufficient to disrupt auditory processing.
The mechanisms are multiple and not fully understood, but current evidence from research into post-traumatic tinnitus points to several sites of disruption:
Direct cochlear trauma
A blow to the head can transmit mechanical force through the skull to the cochlea, causing contusion of cochlear structures, disruption of the basilar membrane, or hemorrhage into the inner ear. This is more likely with impacts close to the ear or involving temporal bone fracture.
Blast injuries, common in military settings, are particularly damaging because the pressure wave enters the auditory canal and strikes the tympanic membrane and middle ear directly while simultaneously transmitting through the skull. VA research documents tinnitus as the single most common service-connected disability in the veteran population, reflecting the high incidence of blast exposure in recent conflicts.
Disruption of the auditory nerve and brainstem
The cochlear nerve (part of the eighth cranial nerve) is vulnerable to traction, shearing, or compression during rapid acceleration-deceleration of the head. Brainstem structures that serve as relay stations for auditory signals, including the inferior colliculus and cochlear nucleus, can sustain diffuse axonal injury from rotational forces even without direct impact.
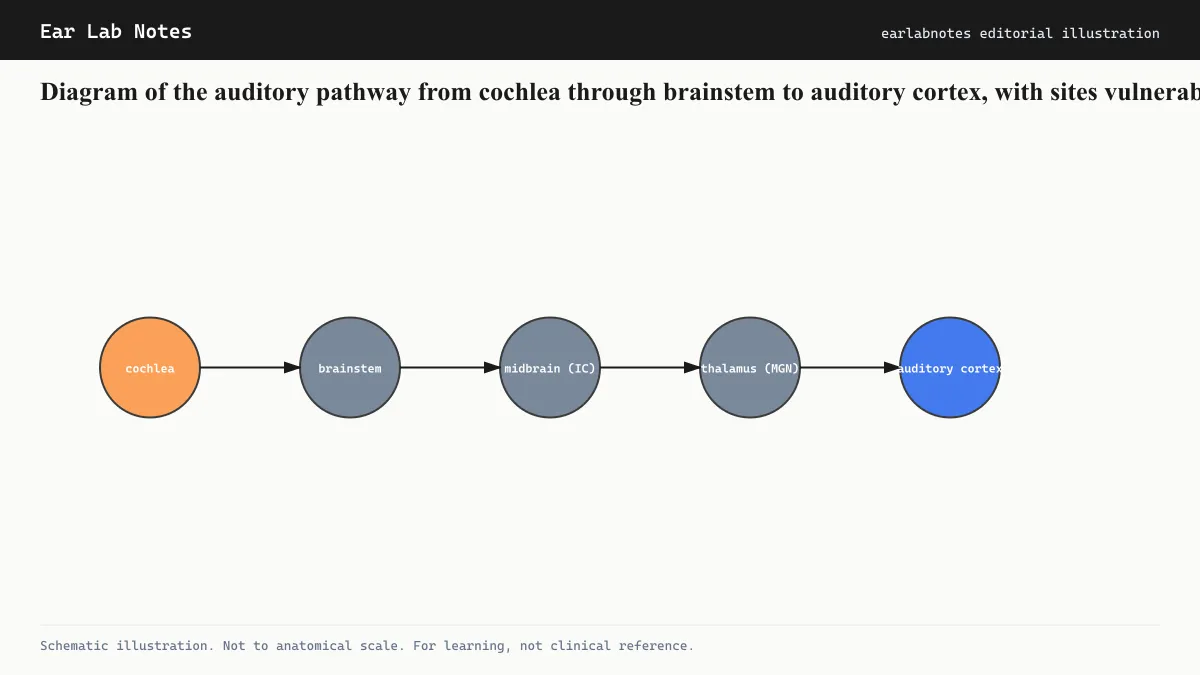
Diffuse axonal injury is a hallmark of mild-to-moderate TBI. It disrupts white matter tracts throughout the brain, including those supporting auditory processing. The result can be changes in the central auditory pathway’s activity that present as tinnitus even when peripheral hearing sensitivity is intact.
Changes in cortical and subcortical auditory processing
Brain imaging studies comparing people with post-traumatic tinnitus to those with tinnitus from other causes have found overlapping but not identical patterns of abnormal activity in the auditory cortex and related limbic structures. Post-traumatic tinnitus is also frequently accompanied by other post-concussive symptoms including headache, cognitive fog, sleep disturbance, and increased emotional reactivity, all of which can interact with and amplify tinnitus distress.
Why audiograms can appear normal
Standard pure-tone audiometry measures the softest tones a person can detect at each frequency. These thresholds depend primarily on inner hair cell function. Outer hair cells, the brainstem relay nuclei, and the cortex are not directly captured.
If a head injury disrupts the central pathway while leaving inner hair cell function largely intact, a person may report tinnitus (and difficulty understanding speech in noise) while their audiogram shows normal thresholds. This phenomenon is related to what researchers call hidden hearing loss or cochlear synaptopathy, where damage affects synapses between hair cells and auditory neurons rather than the hair cells themselves.
For this reason, a normal audiogram after head injury does not rule out clinically meaningful auditory system disruption.
The somatic component
Head and neck injuries also engage somatic tinnitus pathways. The dorsal cochlear nucleus receives somatosensory input from the trigeminal nerve (which innervates the jaw and face) and from dorsal column pathways carrying signals from the upper cervical spine. Trauma affecting the neck, jaw, or temporomandibular joint can activate these pathways and generate or modify tinnitus independently of cochlear damage.
This explains why tinnitus after whiplash injury (without direct head impact) is a recognized clinical entity, and why some people with post-traumatic tinnitus find that their ringing changes when they move their head or jaw.
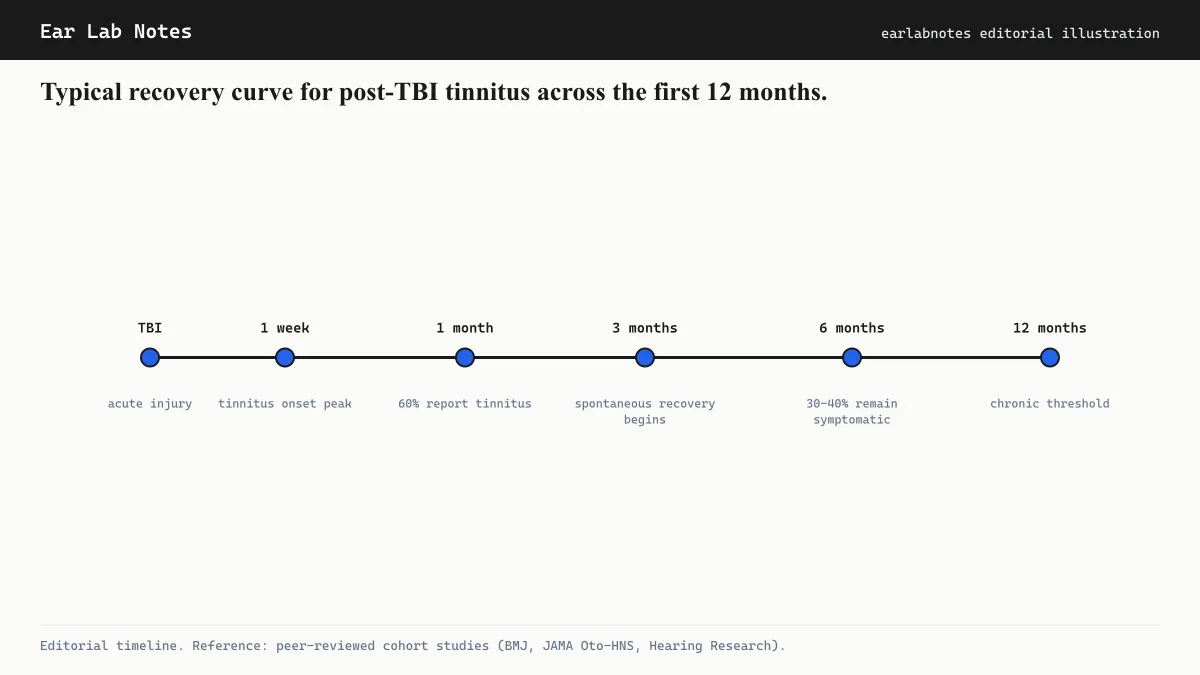
Typical recovery trajectory
The course of post-traumatic tinnitus is variable and difficult to predict for an individual. In general:
Some people experience gradual improvement over the first 3 to 12 months as the nervous system recovers from the acute injury phase. Others find that tinnitus stabilizes at a persistent level. A subset find that tinnitus remains or worsens if other post-concussive symptoms are unmanaged, particularly sleep disruption and psychological distress.
Research in veteran populations suggests that tinnitus associated with PTSD is particularly resistant to resolution and typically requires simultaneous management of both conditions.
There is no treatment proven to accelerate the central auditory pathway’s recovery from trauma-related disruption. Management focuses on reducing the impact of tinnitus on daily function rather than eliminating the signal.
Assessment after head injury
For anyone who develops new tinnitus or worsened hearing after a head injury, a coordinated evaluation is advisable. This typically involves:
- A standard audiogram to assess peripheral hearing thresholds
- Speech-in-noise testing, which can reveal processing difficulties not captured by pure-tone audiometry
- Assessment of vestibular function if dizziness or balance problems accompany the tinnitus
- Screening for cognitive and psychological sequelae of the injury
Depending on findings, referral to audiology, neurology, neuropsychology, or physical therapy (for cervicogenic contributions) may follow.
Management considerations
Post-traumatic tinnitus is managed with many of the same tools used for other forms of tinnitus: sound therapy, cognitive behavioral therapy, and where applicable, treatment of somatic contributors through jaw or neck-focused physical therapy.
Addressing the broader post-concussion picture, including sleep, pain, anxiety, and cognitive function, is generally considered part of tinnitus management in this population rather than a separate undertaking. The AAO-HNS clinical practice guideline on tinnitus does not distinguish post-traumatic tinnitus from other forms in its management recommendations, but clinicians experienced in post-concussion care often tailor the approach to the complexity of concurrent symptoms.
The importance of documentation
For people who develop tinnitus after a documented head injury, early audiological testing establishes a baseline that is valuable for tracking change over time. Insurance, workers’ compensation, and veterans’ benefits systems often require documentation of the temporal relationship between the injury and the onset of tinnitus. An audiogram and clinical record created close to the time of injury is far more useful for these purposes than testing done months or years later.
NIDCD and the American Academy of Audiology both recommend that audiological assessment follow head or ear trauma when any auditory symptoms arise, not only when the hearing loss is obvious.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- I had a concussion six months ago and still have ringing. Is this permanent?
- Post-traumatic tinnitus can persist long after the initial injury, particularly when accompanied by other post-concussive symptoms. While some people see gradual improvement over 12 to 18 months, others do not. An audiologist and a clinician familiar with post-concussion syndrome can assess your specific situation and discuss management options.
- Do I need an audiogram after a head injury?
- Audiological testing after head injury is generally recommended if you notice any change in hearing clarity, new tinnitus, or problems with balance after an impact. An audiogram can identify whether cochlear damage occurred alongside any central auditory disruption, and provides a baseline for tracking change over time.
- Can whiplash alone cause tinnitus without hitting my head?
- Yes. Whiplash-type neck injuries can produce tinnitus through somatic (somatosensory) pathways even when the head itself is not directly struck. The dorsal cochlear nucleus receives input from the upper cervical spine, and disruption of these signals can generate phantom auditory activity.
Primary sources
Where this comes from
- ◆ Tinnitus - NIDCD · National Institute on Deafness and Other Communication Disorders
- ◆ Traumatic Brain Injury Information - NIH · National Institute of Neurological Disorders and Stroke, NIH
- ◆ Tinnitus - Mayo Clinic · Mayo Clinic
- ◆ Clinical Practice Guideline: Tinnitus - AAO-HNS · American Academy of Otolaryngology, Head and Neck Surgery
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N036 · The Ear Lab · earlabs.app