Attention as an amplifier
The auditory system does not passively relay sound to consciousness. It filters, prioritizes, and amplifies based on context and learning. When the brain tags a signal as important, threatening, or novel, that signal receives more processing resources, and it is perceived as louder and more intrusive.
Tinnitus is a phantom signal. It has no acoustic reality in the environment, but within the auditory nervous system it behaves like a real sound. For many people, the first few encounters with tinnitus are alarming, and that alarm recruits the brain’s threat-monitoring circuitry.
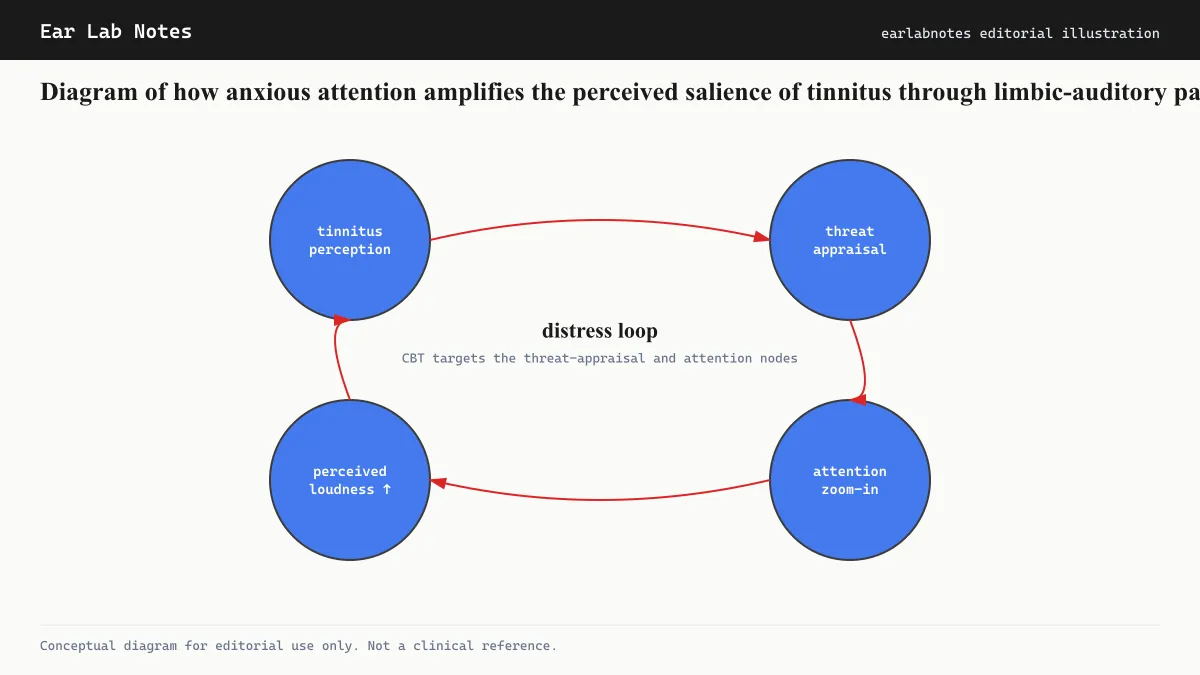
The result is a loop that researchers and clinicians working in tinnitus care have described in detail: anxiety raises auditory attention, which raises perceived tinnitus, which generates more anxiety.
The neuroscience behind the loop
The amygdala’s role
The amygdala is the brain structure most strongly associated with threat detection. When it detects a signal it has learned to associate with threat, it increases arousal and directs attention toward that signal. Research on tinnitus, summarized by NIH/NIDCD-funded groups and others, suggests that in people with high tinnitus distress, the amygdala shows elevated activity in relation to auditory processing, even when the person is not consciously focused on their tinnitus.
This is not a conscious choice. The amygdala operates faster than conscious thought. By the time a person notices they are anxious about their tinnitus, the amplification has already occurred.
Norepinephrine and arousal
Anxiety states increase norepinephrine levels, which is the neurochemical most directly linked to the body’s alert state. Elevated norepinephrine also increases central auditory gain in some neural circuits. This biochemical overlap may be part of why anxiety and tinnitus loudness fluctuate together.
Memory consolidation
Anxiety also affects how strongly memories are consolidated. A tinnitus episode during a high-anxiety period may be encoded more vividly than the same episode during a calm period. Over time, this can mean that the brain’s record of tinnitus is disproportionately weighted toward worst-case encounters.
Who is most affected
Not everyone with tinnitus experiences significant anxiety, and not everyone with anxiety finds that it worsens their tinnitus. The interaction is strongest in people who:
Have anxiety disorders, particularly generalized anxiety disorder, health anxiety, or panic disorder.
Are in the early weeks of tinnitus, when the sound is unfamiliar and its cause and permanence are uncertain.
Have had previous experiences of health-related anxiety, which makes it easier for tinnitus to slot into an existing framework of threat.
Have limited access to information about tinnitus, leaving them to construct explanations that may overestimate the danger the sound represents.
Why anxiety makes clinical management harder
Tinnitus management generally aims at habituation: the process by which a persistent but non-threatening stimulus is progressively ignored by the brain. Habituation requires the limbic system to reclassify the signal as non-threatening.
Anxiety actively prevents this reclassification. A brain in an anxious state monitors for threats; it cannot simultaneously reclassify a signal as safe. This is why clinicians who work with tinnitus patients frequently note that anxiety treatment is a prerequisite for successful habituation in people with comorbid anxiety.
The AAO-HNS clinical practice guideline for tinnitus acknowledges the psychological dimension of management and supports referral to appropriate mental health providers when anxiety or depression are present.
What cognitive behavioral therapy does
CBT for tinnitus targets the threat appraisal at the center of the anxiety-tinnitus loop. Sessions typically involve:
Identifying automatic thoughts about tinnitus, such as beliefs that it will worsen, cause deafness, or be permanent.
Examining those beliefs against available evidence.
Practising attention redirection so that sustained monitoring of the phantom sound is gradually reduced.
Behavioral experiments that reduce avoidance of situations where tinnitus might be noticeable.
Multiple controlled trials and systematic reviews have found that CBT reduces tinnitus handicap scores and anxiety measures, often concurrently. The British Tinnitus Association and NHS UK both list CBT as a recommended approach for tinnitus distress.
Sound enrichment as an anxiety-reduction tool
Providing a background of non-threatening environmental sound reduces the contrast that makes tinnitus salient. Many people find this also reduces the anxiety spike that comes from noticing the phantom sound suddenly in a quiet room.
Sound enrichment is not a cure and does not change the underlying tinnitus. It changes the context in which the sound is perceived, which can interrupt the first step of the anxiety loop.
Practical strategies that do not require a clinical referral
While professional support is the recommended route for significant anxiety and tinnitus, several strategies are consistent with what clinicians advise and can be incorporated into daily life:
Sound enrichment in quiet environments. Keeping some acoustic background, a fan, nature sounds at low volume, or a radio in another room, reduces the contrast that makes tinnitus salient and lowers the spike of anxiety that comes from suddenly noticing silence.
Limiting checking behaviors. Repeatedly testing whether tinnitus is louder, covering one ear to compare, or searching for changes sustains the monitoring that feeds the anxiety loop. Reducing checking is a behavioral element of most CBT-for-tinnitus protocols.
Structured relaxation practice. Progressive muscle relaxation and slow breathing techniques reduce general arousal, which lowers the baseline state in which tinnitus is perceived. These are not tinnitus treatments, but they change the physiological context in which tinnitus is heard.
Sleep hygiene. Anxiety is substantially worsened by poor sleep, and tinnitus is a common disruptor of sleep. Attending to sleep onset conditions, consistent schedule, and a modest acoustic background at night can reduce both the anxiety and the tinnitus salience that drives it.
What to expect if you seek help
An audiologist assessing tinnitus with a significant anxiety component will often administer validated questionnaires such as the Tinnitus Handicap Inventory and may also screen for anxiety using standardized tools such as the Generalized Anxiety Disorder scale (GAD-7). The results help determine whether psychological referral is appropriate alongside audiological management.
The AAO-HNS clinical guideline and NHS tinnitus pathways both support referral to psychological services when anxiety is a prominent feature of tinnitus distress. In many health systems, structured group CBT programs for tinnitus are available at lower wait times than individual therapy, and some have been delivered effectively in online formats.
A GP or mental health provider familiar with chronic conditions can assess anxiety independently. Coordinated care between audiology and mental health tends to produce better outcomes than either alone, because the two conditions are mechanically linked and each influences how well the other responds to treatment.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- Can anxiety cause tinnitus?
- Anxiety does not appear to generate tinnitus where none existed before. However, anxiety strongly influences how prominent existing tinnitus feels. High anxiety states direct attention toward potential threats, and tinnitus can become one of those threats, increasing perceived loudness and intrusiveness.
- Why does my tinnitus seem worse when I am anxious?
- Anxiety triggers the body's threat-response system, which heightens alertness and focuses attention on potential danger signals. If the brain has learned to monitor tinnitus as something worth watching, that heightened state will make the phantom sound feel more prominent, even if its actual acoustic level has not changed.
- Is tinnitus a symptom of anxiety disorder?
- Tinnitus is not listed as a diagnostic symptom of anxiety disorders. However, the two conditions frequently co-occur. People with generalized anxiety disorder or panic disorder who also have tinnitus often report greater tinnitus distress than those without an anxiety condition.
- What helps break the tinnitus-anxiety cycle?
- Cognitive behavioral therapy is the most evidence-supported approach for both tinnitus distress and anxiety. It works partly by changing the threat appraisal that sustains the attention-amplification loop. Mindfulness-based approaches have also shown benefit in some studies.
- Should I avoid quiet rooms if I have tinnitus and anxiety?
- Complete silence tends to make tinnitus more noticeable, which can spike anxiety in people prone to that loop. Many people find a low-level background sound helpful in quiet settings. A qualified audiologist or therapist can help tailor this to individual circumstances.
Primary sources
Where this comes from
- ◆ Tinnitus: Assessment and Management · NIH/NIDCD
- ◆ Tinnitus Clinical Practice Guideline · AAO-HNS
- ◆ Tinnitus and mental health · British Tinnitus Association
- ◆ Tinnitus: Symptoms and causes · Mayo Clinic
- ◆ Tinnitus overview · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N037 · The Ear Lab · earlabs.app