Most tinnitus is bilateral. It rings, buzzes, or hisses in both ears, or somewhere in the middle of the head. When tinnitus is clearly one-sided, confined to a single ear and heard distinctly from that location, it sits in a different clinical category.
Unilateral tinnitus accounts for a minority of all tinnitus presentations. The AAO-HNS (American Academy of Otolaryngology) clinical practice guideline on tinnitus lists unilateral, pulsatile, or rapidly worsening tinnitus among the presentations that should prompt formal medical evaluation rather than watchful waiting.
That does not mean the cause is always serious. The majority of unilateral tinnitus cases have benign explanations. But some causes are treatable, and a small number are medically significant. That asymmetry is why clinicians treat one-sided ringing differently from the typical bilateral presentation.
Why laterality matters
The auditory pathway is largely bilateral from early in its course. Sound entering the right ear is processed not just in the right auditory cortex but distributed across both hemispheres fairly quickly. Fully bilateral tinnitus, generated centrally after cochlear damage, generally matches this pattern.
When a patient reports consistent tinnitus in one ear only, it raises the question of a structural or pathological process that is lateralized to one side. The inner ear, auditory nerve, or structures immediately adjacent to them on one side may be involved.
Common causes of one-sided ringing
Asymmetric or unilateral hearing loss
The most frequent explanation for unilateral tinnitus is asymmetric hearing loss, where one ear has notably worse thresholds than the other. This can follow unilateral noise exposure (holding a phone to one ear, occupational exposure from one direction), a single-sided ear infection, or progressive conditions that affect one side more than the other.
Audiometry is the essential first test. If thresholds differ significantly between ears, that asymmetry itself requires explanation.
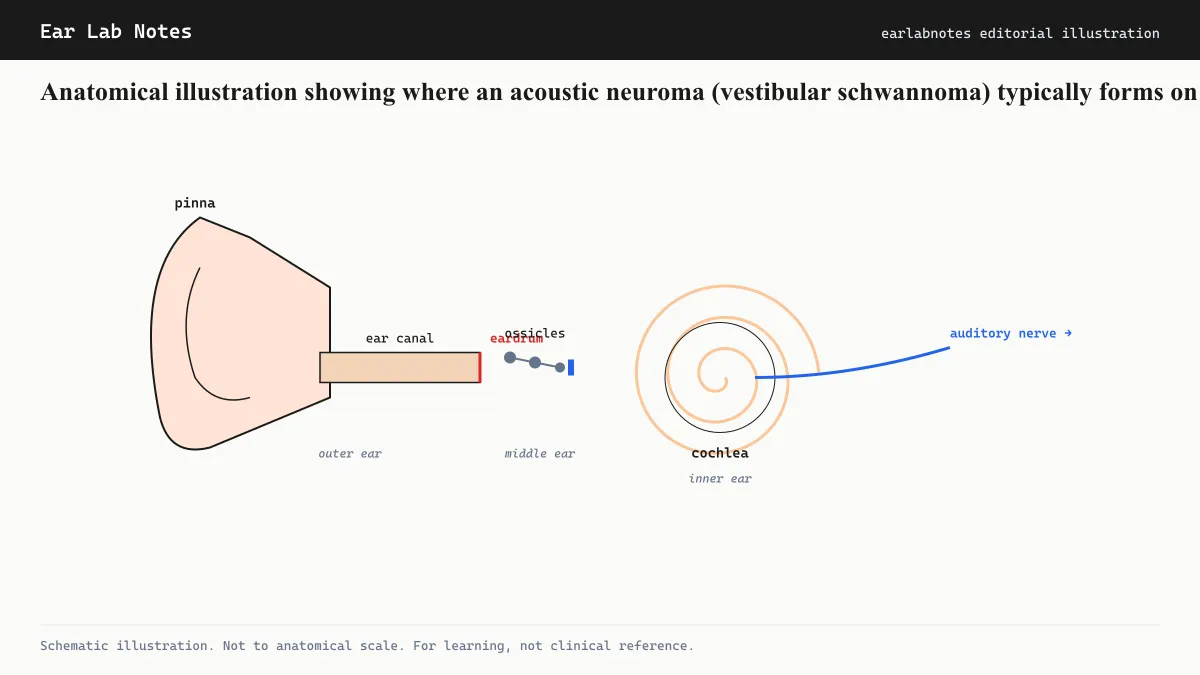
Acoustic neuroma (vestibular schwannoma)
An acoustic neuroma is a benign, slow-growing tumor on the vestibular branch of the eighth cranial nerve. It sits in the internal auditory canal, a bony channel through which the auditory and vestibular nerves travel from the inner ear to the brainstem.
As the tumor grows, it can compress the auditory nerve, producing unilateral tinnitus, unilateral sensorineural hearing loss, and sometimes vertigo or imbalance. The NIDCD notes that acoustic neuromas are uncommon (roughly 1 in 100,000 per year), but tinnitus is among their presenting symptoms in a substantial proportion of cases.
Because acoustic neuromas are slow-growing and benign, the concern is not immediate danger but rather early detection while the tumor remains small and management options are broader. The Mayo Clinic notes that treatment options include monitoring, radiosurgery, and microsurgery depending on size and growth rate.
Meniere’s disease
Meniere’s disease is characteristically unilateral, at least in its early stages. It produces fluctuating low-pitched tinnitus, episodic vertigo, a sensation of fullness in the ear, and fluctuating hearing loss. The tinnitus often shifts in pitch and volume around vertigo episodes.
About 15 percent of Meniere’s cases eventually become bilateral, but the initial presentation is typically confined to one ear.
Sudden sensorineural hearing loss
Sudden sensorineural hearing loss (SSNHL) is defined as rapid hearing loss of at least 30 dB across three consecutive frequencies over 72 hours or less. It almost always affects one ear. Tinnitus in that ear frequently accompanies the sudden hearing loss.
SSNHL is considered a medical emergency. If it occurs alongside new unilateral tinnitus, prompt evaluation is critical, as some causes are treatable if addressed quickly.
Earwax and middle-ear conditions
Impacted cerumen, middle-ear fluid (otitis media with effusion), or a perforated eardrum on one side can produce conductive tinnitus that is unilateral. These are benign causes, and in many cases the tinnitus resolves when the underlying condition is addressed.
The clinical workup
The AAO-HNS guideline recommends formal evaluation of unilateral tinnitus, typically beginning with audiometry. If the audiogram shows asymmetric sensorineural hearing loss, or if the tinnitus is accompanied by other concerning features (vertigo, sudden onset, pulsatile quality), the next step is typically MRI of the internal auditory canals with gadolinium contrast.
This imaging is specifically designed to identify acoustic neuromas and other soft-tissue abnormalities along the auditory pathway.
What “asymmetric hearing loss” means on an audiogram
Audiologists look for a difference in thresholds of 15 dB or more at two or more consecutive frequencies between the two ears, or a 15 dB or greater difference in word recognition score. These thresholds vary slightly by guideline, but the principle is consistent: significant between-ear differences need explanation.
A normal audiogram does not completely rule out a small acoustic neuroma or cochlear synaptopathy. MRI remains the definitive test when clinical suspicion is high.
When to seek evaluation promptly
The NHS UK and AAO-HNS both identify circumstances where tinnitus, including unilateral presentations, warrants prompt rather than deferred evaluation:
- Sudden onset of tinnitus accompanied by sudden hearing loss
- Unilateral tinnitus with vertigo or balance disturbance
- Tinnitus following head trauma
- Pulsatile tinnitus (tinnitus that beats in time with the pulse)
- Any tinnitus associated with neurological symptoms
Chronic, stable, unilateral tinnitus with a clear audiometric correlate is lower urgency, but still warrants a formal assessment rather than self-monitoring alone.
If symptoms persist or change, see an audiologist or physician.
Related notes
Frequently asked
Questions readers ask
- Is tinnitus in one ear always serious?
- Not always, but unilateral tinnitus is considered a clinical red flag and warrants evaluation by an audiologist or otolaryngologist. The majority of cases turn out to have a benign explanation, but imaging is typically recommended to rule out acoustic neuroma and other treatable causes.
- What is an acoustic neuroma?
- An acoustic neuroma, more precisely called a vestibular schwannoma, is a benign (non-cancerous) tumor that grows on the vestibular branch of the eighth cranial nerve. It is slow-growing and rarely life-threatening, but it can compress adjacent structures and affect hearing and balance if left undetected. It is one of the primary reasons clinicians take unilateral tinnitus seriously.
- How is unilateral tinnitus diagnosed?
- Evaluation typically begins with a detailed history and a full audiogram. Audiologists look for asymmetric hearing loss, which can accompany unilateral tinnitus. If asymmetry is found, or if the presentation otherwise raises concern, the next step is usually MRI with gadolinium contrast to image the internal auditory canals.
- Can earwax cause tinnitus in just one ear?
- Yes. Impacted cerumen (earwax) in one ear can produce a conductive tinnitus in that ear alone. This is one of the more benign and easily reversible causes. An otolaryngologist or general physician can assess and safely remove impacted wax if present.
Primary sources
Where this comes from
- ◆ Clinical Practice Guideline: Tinnitus · American Academy of Otolaryngology - Head and Neck Surgery (AAO-HNS)
- ◆ Acoustic Neuroma · NIH/NIDCD
- ◆ Vestibular Schwannoma (Acoustic Neuroma) · Mayo Clinic
- ◆ Tinnitus: causes and management · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N046 · The Ear Lab · earlabs.app