Tinnitus is the perception of sound when no external sound source is present. Most people describe it as ringing, but it can also sound like hissing, buzzing, clicking, roaring, or pulsing. According to NIDCD, roughly 10 percent of American adults experience some form of tinnitus, making it one of the most common sensory complaints in medicine.
Understanding what produces tinnitus requires separating two questions: where does the abnormal activity originate, and why does the brain interpret it as sound? Researchers have identified four broad mechanisms. They are not mutually exclusive, and many people with tinnitus have more than one at play.
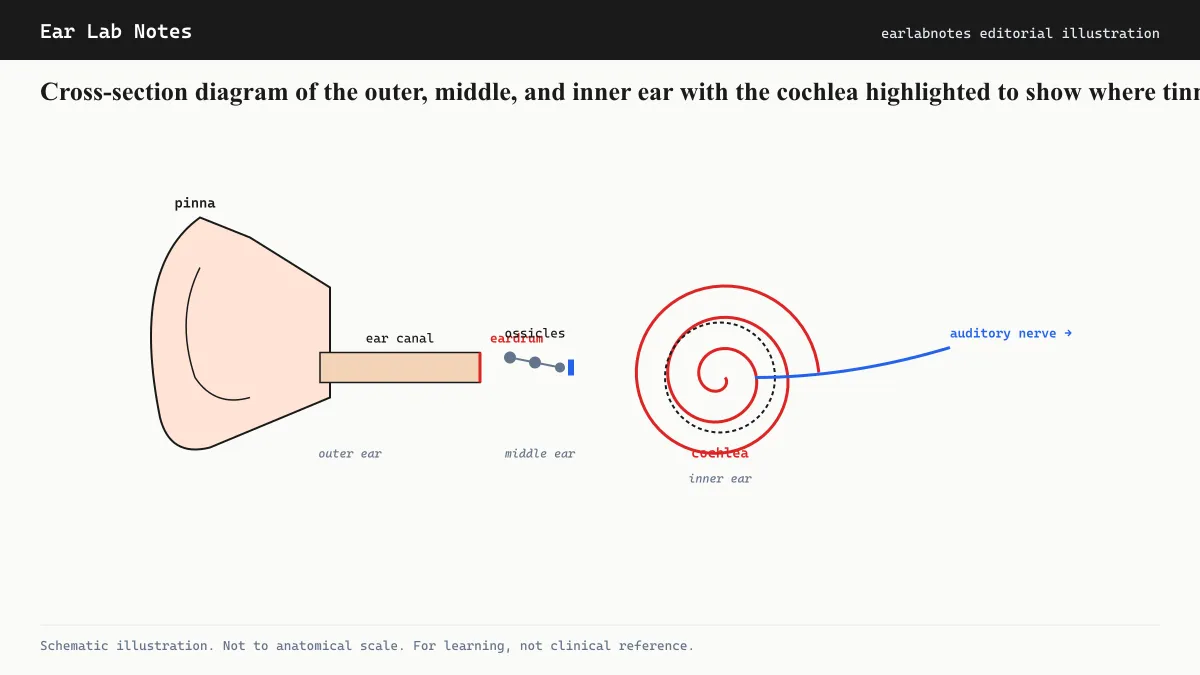
Mechanism 1: Cochlear hair-cell damage
The inner ear contains roughly 16,000 sensory hair cells arranged along the cochlea. Their job is to convert mechanical vibrations into electrical signals the auditory nerve can carry to the brain. Each hair cell is tuned to a specific frequency, a property called tonotopy.
When hair cells are damaged, by noise, aging, certain medications, or infection, the corresponding nerve fibers lose their normal input. The current leading hypothesis, sometimes called the central-gain model, holds that the brain’s auditory pathway compensates for this reduced input by increasing its own internal amplification. That amplified internal noise becomes perceptible as tinnitus.
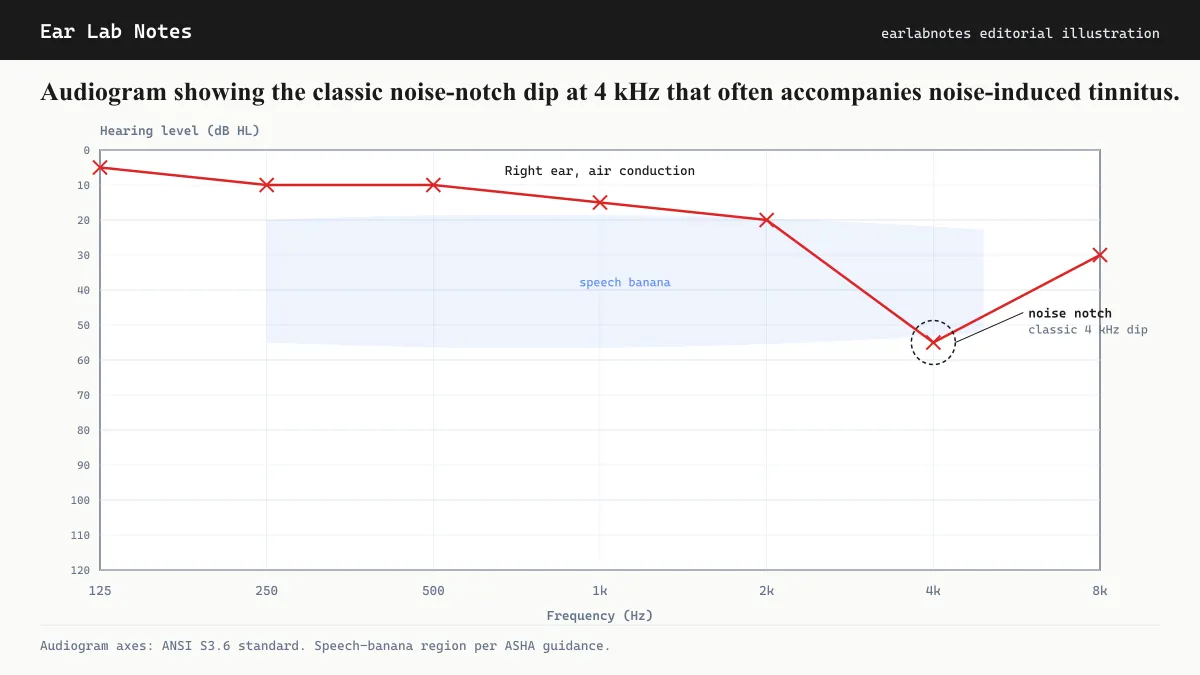
NIDCD notes that noise-induced hearing loss is the single most common identifiable cause of tinnitus. The hair cells most vulnerable to noise sit at the base of the cochlea, which is tuned to high frequencies, which is why noise-induced tinnitus is most often perceived as a high-pitched ringing.
Hair cells in humans do not regenerate once destroyed. This is a key reason why tinnitus from significant cochlear damage tends to persist.
Mechanism 2: Neural plasticity and central reorganization
Even when cochlear damage is mild or absent, the auditory cortex and subcortical auditory nuclei can generate aberrant activity that presents as tinnitus. This is sometimes called central tinnitus.
When input from a region of the cochlea is reduced, neighboring neurons in the auditory cortex can expand their receptive fields to cover the silent zone. This maladaptive reorganization, a feature of brain plasticity turned harmful, is associated with spontaneous firing in the deprived region. That spontaneous firing has no external source, but the brain processes it as sound.
Brain-imaging research using fMRI and magnetoencephalography has detected measurable differences in auditory cortex activity in people with chronic tinnitus compared to those without it, even when standard audiograms show no hearing loss. These findings support the view that tinnitus can be a brain-level phenomenon rather than purely an ear-level one.
Mechanism 3: Somatic input from the jaw and neck
A distinct subgroup of people have tinnitus that changes in quality, pitch, or loudness when they move their jaw, press on their neck muscles, or change their eye position. This is called somatic or somatosensory tinnitus.
The dorsal cochlear nucleus, a brainstem relay station in the auditory pathway, receives input from somatosensory nerves in the jaw and neck alongside its normal auditory input. When somatosensory signaling is abnormal, as it can be after whiplash, jaw misalignment, or temporomandibular joint (TMJ) disorders, that aberrant input may drive the dorsal cochlear nucleus to generate phantom auditory activity.
This mechanism is important clinically because it points toward different assessment and management strategies compared to cochlear tinnitus.
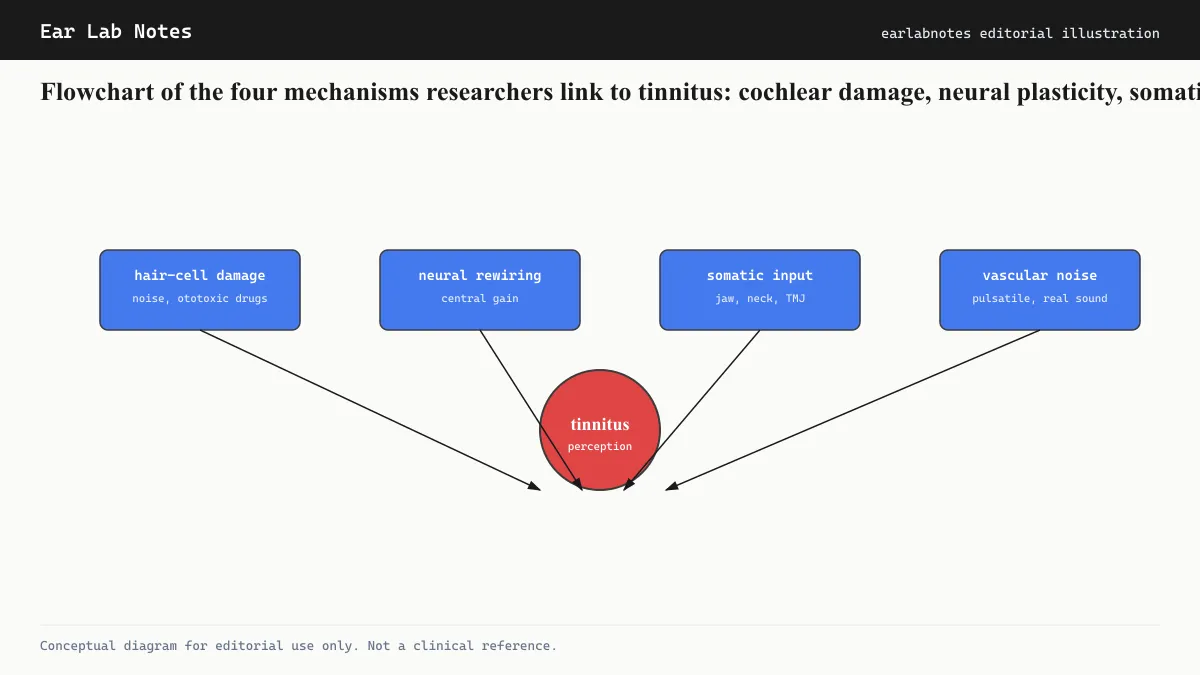
Mechanism 4: Vascular noise
A small percentage of tinnitus cases are caused by actual sound generated within the body, transmitted to the ear through surrounding tissue rather than perceived as phantom sound. The most recognized form is pulsatile tinnitus, where the person hears a rhythmic sound synchronized with their heartbeat.
The structures most commonly involved are the carotid artery and the jugular vein, both of which pass close to the middle and inner ear. Conditions that alter blood flow, including high blood pressure, atherosclerotic narrowing, arteriovenous malformations, and elevated pressure in the fluid around the brain, can make the sound of turbulent blood flow audible.
Unlike the other three mechanisms, vascular tinnitus is sometimes categorized as objective because, in principle, a clinician with a stethoscope or microphone placed near the ear can occasionally detect the same sound. This distinction matters for workup because vascular causes may require imaging and targeted treatment rather than audiological management alone.
How these mechanisms interact
Many people with tinnitus have overlapping mechanisms. Someone with significant noise-induced cochlear hair-cell damage may also have central reorganization compounding the peripheral signal. A person with a jaw injury may have both somatic input driving the dorsal cochlear nucleus and concurrent noise-related cochlear changes.
This overlap explains why tinnitus can persist even when the initial trigger is addressed, and why effective management often requires addressing multiple components.
What tinnitus is not
Tinnitus is not a disease in itself. It is a symptom, the auditory equivalent of pain. Just as pain indicates that something requires attention without specifying exactly what, tinnitus indicates disruption somewhere in the auditory system without defining the diagnosis.
The AAO-HNS clinical practice guideline on tinnitus distinguishes between primary tinnitus (no identifiable underlying cause beyond possible hearing loss) and secondary tinnitus (associated with a specific, identifiable condition such as Meniere’s disease, acoustic neuroma, or ototoxic medication use). Secondary forms may resolve if the underlying cause is treated.
The role of attention and emotional response
The perceived loudness of tinnitus does not always match its objective signal strength. Research in cognitive psychology and audiology shows that attentional focus and emotional state substantially modulate how intrusive tinnitus feels. This is not a suggestion that tinnitus is “in the head” in a dismissive sense; it is a statement about how the brain’s evaluative systems shape perception of any signal.
Understanding this mechanism is important because it underlies why psychological interventions, particularly cognitive behavioral therapy, have the strongest evidence base of any tinnitus intervention according to systematic reviews. Changing the response to tinnitus, rather than eliminating the signal, is the most consistently effective approach currently available.
How common is tinnitus, and who is most affected
NIDCD estimates that about 10 percent of American adults experience tinnitus lasting at least five minutes in the past year. Roughly 1 in 4 of those find it at least somewhat bothersome, and about 20 million people in the United States experience chronic tinnitus. NHS UK data suggest broadly similar prevalence in the UK population.
The condition is more common in:
- People over 60, because age-related cochlear hair cell loss (presbycusis) is cumulative and nearly universal
- People with occupational or recreational noise exposure histories
- Current or former military personnel, given the combination of blast exposure and occupational noise
- People taking medications with known ototoxic profiles
- People with cardiovascular risk factors, because vascular health affects cochlear circulation
Tinnitus is not a condition that exclusively affects older adults. Noise exposure in younger populations, including through recreational music and earbuds, is a growing concern that NIDCD and NIOSH have highlighted in public health communications.
When to seek evaluation
NIDCD and NHS UK both recommend seeking medical evaluation for tinnitus that is new, persistent (lasting more than a week), accompanied by hearing loss or dizziness, present in only one ear, or pulsatile. These features help clinicians distinguish primary tinnitus from secondary forms that may have a treatable cause.
A standard tinnitus evaluation typically includes a detailed history, physical examination of the ears, and a pure-tone audiogram. Depending on findings, additional testing such as imaging or vestibular assessment may follow.
If symptoms persist or change, see an audiologist or physician.
Related notes
Watch
Mayo Clinic Minute: Is tinnitus causing that ringing in your ear?
Source: Mayo Clinic on YouTube
Transcript / summary
Frequently asked
Questions readers ask
- Is tinnitus always caused by loud noise exposure?
- No. Loud noise is one of the most common triggers, but tinnitus can also result from earwax blockage, certain medications, jaw disorders, blood pressure changes, and other conditions. An audiologist or physician can help identify the likely cause in your specific case.
- Can tinnitus go away on its own?
- Acute tinnitus after a loud noise event (such as a concert) often fades within hours or days. Chronic tinnitus, defined roughly as lasting more than three months, is less likely to resolve spontaneously. The trajectory varies considerably depending on the underlying cause.
- Is tinnitus a disease or a symptom?
- Tinnitus is a symptom, not a disease in itself. According to NIDCD, it indicates that something in the auditory system is not working as it should, but it can arise from many different underlying conditions.
- Should I be worried if I have tinnitus in only one ear?
- One-sided tinnitus is considered a clinical red flag by AAO-HNS guidelines, because it warrants evaluation to rule out uncommon but treatable causes such as acoustic neuroma. A visit to an audiologist or otolaryngologist is advisable.
Primary sources
Where this comes from
- ◆ Tinnitus - NIDCD · National Institute on Deafness and Other Communication Disorders
- ◆ Tinnitus - Mayo Clinic · Mayo Clinic
- ◆ Clinical Practice Guideline: Tinnitus - AAO-HNS · American Academy of Otolaryngology, Head and Neck Surgery
- ◆ Tinnitus - NHS · NHS UK
Educational use only.
If your symptoms persist or change, see a licensed audiologist or otolaryngologist. Sudden hearing loss is a medical emergency, see a clinician within 72 hours.
TEL—N047 · The Ear Lab · earlabs.app